
Advice
A friend of mine in Seattle told me that they’d gotten COVID-19, and asked me what they should do next. What could they do to get better sooner/faster/better? How should she protect their partner? This is the advice I gave:
- Stay away from your partner until you test negative.
- Stay entertained.
- Paxlovid, if appropriate.
- Irrigate your sinuses.
- Make sure you have clean air.
- Be quiet.
- Don’t try to do too much when you spring yourself.
Isolate until you test negative
The US CDC says to isolate until five days after your first symptoms. The BC CDC says that if you are fully vaccinated, you can stop isolating after five days if your symptoms improve and you don’t have a fever. This is utter bullshit. There are lots of studies which say that most people are still infectious until 7-10 days after symptom onset:
- This preprint from the USA (with samples taken during the early Alpha period) found they could grow viral culture from participants for a mean of 11 days;
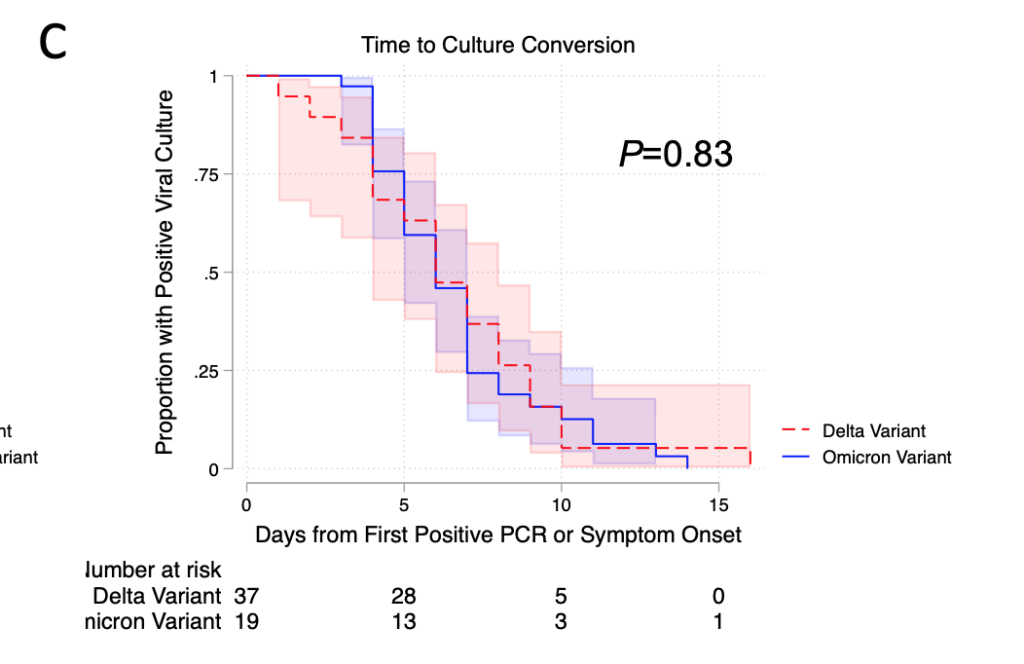
- This preprint from the UK (with samples taken during the Delta/B.1/B.2 period) found that people had high enough viral load to be infectious for 7-10 days. They found no correlation of symptom severity with viral load.
- This preprint from the USA (with samples taken from July 2021 to January 2022) found a median of 6 days from positive test or start of symptoms to no longer cultureable, although 15% of participants’ swabs could culture virus for more than 10 days.

I believe that I have seen more papers than the three mentioned, but they are a little hard to search for.
Stay entertained
Early in the pandemic, I used to say, “It turns out that love is stronger than fear” as people broke quarantine rules around the world to spend time with loved ones. Now, I say, “Boredom is stronger than fear” as I have seen people I know go places after five days, even knowing that they were probably still infectious after five days. (They knew because I told them.)
I also have isolated twice, once early on when I had symptoms and once recently when I was exposed. It’s hard!
So one of the most important things you can do to keep from infecting your loved ones is to stay isolated! And you aren’t going to be able to do that if you are bored out of your skull and/or frantic for physical exercise. If you have someone to help take care of you, have them bring you stuff. Better yet, arrange this ahead of time. (See later on for my ‘how to prepare’ list.)
Walking around outside, especially if you have a mask on, is relatively low risk for other people. (Don’t do this if you are sneezing or coughing, though. You won’t be able to restrain yourself from lifting your mask to cough/sneeze (because yeah, that’s gross), but that’s exactly the time when the mask is needed.) Do wear a mask when going from your room to the door, and preferably have your roommates be far away. (I can’t go outside when isolating because I live in an apartment building where I can’t get up to my floor without getting into a small poorly ventilated room an elevator.)
Paxlovid
If you are eligible for Paxlovid (BC rules, USA rules), and don’t have drug interactions which would conflict, get on the phone immediately to your doctor. Paxlovid works really well.
Irrigate your sinuses
Irrigating your sinuses (with something like this) works even better than Paxlovid. No lie. (I’m not saying do it instead of Paxlovid. Do both.)
- This paper found that irrigating sinuses with saline or povidone-iodine after getting infected cut the hospitalization rate in people over 55 by 8.57 TIMES. Not 8.6%, 8570% percent. They saw no difference between saline and povidone-iodine.
- This paper on a study of hospital workers in Mexico (I think in late 2019/early 2020) found that 1.2% of workers who did nasal rinses with neutral electrolyzed water got COVID-19, compared to 12.7% in the control group who did.
- This paper found that people who irrigated with saline got over COVID-19 symptoms in about 10 days vs. 14 days for people who didn’t.
- This small study from France early in the pandemic found that after sinus rinse with povidone iodine (not saline!) all the COVID-19 patients in the study but one tested negative after three days.
- This paper doesn’t give results, it just tries to explain what the helpful actions of nasal irrigation are (at a cellular level).
- This small study pre-pandemic of people with “common colds” found that people who did nasal irrigation and gargled resolved symptoms 1.9 days before those who did not and reduced household transmission by 35%. (Note that many “common colds” are coronaviruses!)
I have had a number of people express extreme hesitancy about sinus irrigation. “I remember getting salt water / pool water up my nose, and it was horrible!” Yes! Getting salt water / pool water / tap water up your nose is absolutely horrible. 0/10, would not do again. However, the salt + baking soda that you put in your irrigation water means that it doesn’t hurt at all. It’s a little weird, but it does not hurt. (You do want to use distilled water or boiled water.)
Addendum: probiotics
Added on 2 Dec 2022: There are now a number of papers which say that the gut biome gets messed up by COVID-19. Several explicitly say that taking probiotics is useful. See this Twitter thread for a summary of papers.
Make sure your air quality is good
There have been lots of studies which have shown that air pollution (like, oh, say, smoke from wildfires) is really bad for COVID-19, and the effects are not small. When air quality in an area is poor, more people catch COVID-19 and they have more severe cases. The studies disagree on which aspect of the air pollution is most responsible, but they all say air pollution IS BAAAAAD:
- This paper from China says air pollution is bad, humidity is good.
- This paper from Iran says that air pollution is bad for COVID-19, with different correlations at different times.
- This paper from the USA says that each 4.6ppb increase in NO2 made the COVID-19 case-fatality rate and mortality rate go up by 11.3%; a 2.6 μg/m increase in PM2.5 made the mortality rate go up by 14.9%.
- This paper from the USA says that “an increase in the respiratory hazard index is associated with a 9% increase in COVID-19 mortality”.
- This paper from China found that a 10-μg/m3 increase in PM2.5, PM10, NO2, and O3 was associated with a 2.24%, 1.76%, 6.94%, and 4.76% increase in the daily counts of confirmed cases.
- This paper using data from China, Italy, and the USA found that NO2 correlated with per capita cases (tau .12-.52, depending on the country). PM2.5 had a weaker correlation (tau .08-.31). PM2.5 correlated to mortality (tau .14-.19)
- This paper from Italy says that “long-term air-quality data significantly correlated with cases of Covid-19 in up to 71 Italian provinces”.
- This paper from the USA says that “an increase of only 1 μg/m3 in PM2.5 is associated with an 8% increase in the COVID-19 death rate”
I bumped into this paper from the USA which talked about how nasty the air is in open-kitchen restaurants. Apparently, grilling and frying meat gives off a ton of particles. (This makes sense; it sometimes gets smoky in the kitchen when you are cooking. Those are particles!) This explained something which I had heard but didn’t understand: line cooks have the highest mortality of all the occupations. You’d think it would be meatpackers or health care workers, but no. Cooking makes particles, and PARTICLES ARE BAD FOR COVID-19!
I am not a doctor, but the picture I have put together is that the cilia in the respiratory tract are like little conveyor belts which take crud out. If your cilia get gunked up with soot, then they can’t take out the COVID-19 viruses as well. Similarly, if they are full of COVID-19, when you do a nasal rinse, you take out a bunch of the garbage for them, and make it easier for them to take the rest of the garbage out. Help your cilia! Reduce the amount of gunk you breath in and rinse gunk out!
If you need more proof that air quality is important, check out this tweet: air pollution is the fourth-leading risk factor for death:

Be quiet
There was one paper which said that they couldn’t find any culturable virus from the breath of people who were “tidal breathing”, i.e. just sitting there, not exercising, not talking / singing / yelling / coughing / sneezing.
Take it easy!
There was one kind of throw-away sentence in an abstract of a study on Long COVID which said that not taking it easy after recovering from COVID-19 correlated with getting Long COVID. I remember that, but I’m sorry to say that I can’t find the paper.
It was only one paper, and I don’t know how they justify the claim. However, it makes sense to me, is relatively cheap and easy to do (compared to like, spending a week in a hyperbaric pressure chamber or something like that), and has very few side effects.
Get prepared ahead of time
Once you are sick, there are things I mention above which you will not be able to do for yourself. If you have family or friends who will take care of you, you can offload some stuff to them, but it’ll be easier if you prepare ahead of time. If I were you, and you can, I would make sure you have these on hand:
- High-quality N95-class masks. These will help keep your household members safe if you have to make brief dashes into common areas. They will also help you if the air quality sucks and you don’t have an air filtration device.
- Sinus irrigation kit and 4 litres of distilled water. The NeilMed kits are about CAD$20 at just about any pharmacy. Yes, they are a total rip-off — twenty bucks for a plastic bottle and some salt and baking soda?!?!? However, their value is much higher than their price.
- If you can find another bottle that will work, good for you, use that. Put equal parts baking soda and salt into a bottle, shake really really well, and put 1/4 teaspoon into 250 ml of water, and irrigate away.
- Particle detector and air filtration device. This is the particle detector I got, though I got it from the US.
- Spouse and I built a Corsi-Rosenthal box (cost ~CAD$200) which works really well. During the recent wildfire smoke, it took the PM2.5 count in our living room from 47 µg/m^3 to 12 µg/m^3 in 17 minutes. (NB: I had a hard time finding a 20″ box fan on short notice when we were making ours.)
- Here’s a mini Corsi-Rosenthal box.
- Here’s a tweet thread talking about making a thinner box with computer fans.
- Entertainment. Netflix? Books? Art supplies? Videogames? This is going to be highly individual.
- Physical activity equipment. This might be weights, a jump rope, a hula-hoop, a stepstool, dancercize videos, Wii, whatever. Just something that will help you move your muscles a little.
Transmission
A lot of people are sick these days “but not with COVID-19, because I tested negative”. This tweet reports that Alberta wastewater — where they test for influenza, RSV, and COVID-19 — shows 100x as much COVID-19 as flu or RSV. Me, I think the rapid tests are probably wrong: probably “everybody” has COVID-19.
Mitigation Measures
This paper from the US says that 40% of the people there lied about their adherence to measures and/or broke the rules. “The most common reasons included wanting life to feel normal and wanting to exercise personal freedom.”
This article reports that Canadian Armed Forces is dropping a vaccine mandate. They are still going ahead with expelling some service personnel who did not get vaccinate. (I guess that makes sense: they are getting thrown out not for being unvaccinated, but for disobeying orders.)
Long COVID
A StatCan report says that
- 32% of Canadians were sure they’d had COVID-19, and another 8.3% suspected it;
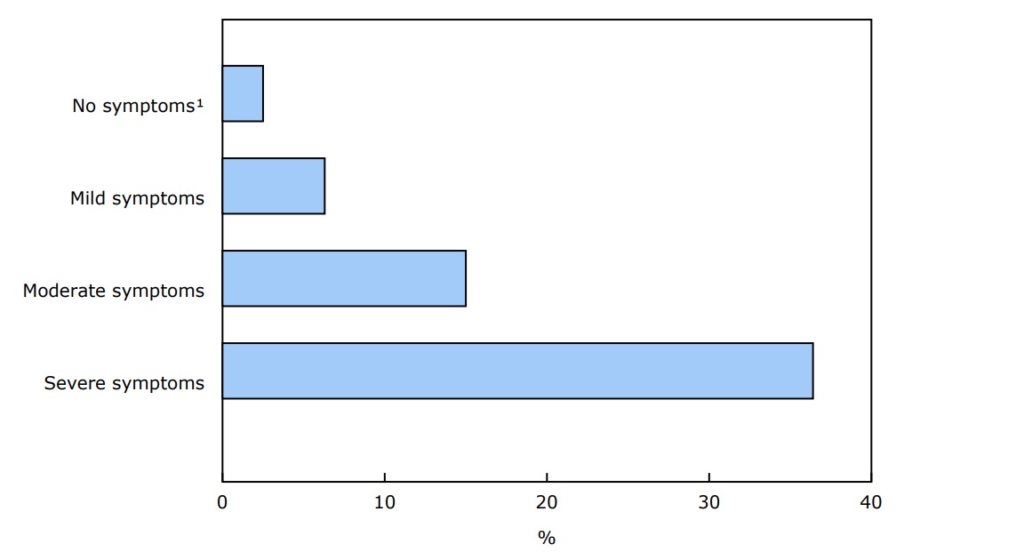
- 16.7% of people who’d had COVID-19 reported having severe symptoms;
- 14.8% of them had symptoms for at least three months;
- 36.4% people who had severe symptoms had symptoms at three months;
- 25.8% of people who caught it before Dec 2021 (i.e. pre-Omicron) had symptoms at three months;
- 10.5%. of people who caught it after Dec 2021 (i.e. who probably got Omicron) had symptoms at three months;
- 32.5% of the people who’d had COVID-19 said that they thought they were all recovered, then they rebounded.
This article from the USA talks about the promise of low-dosage naltrexone — usually used as anti-addiction medication — against Long COVID.
This paper from Canada looked at people who had had COVID-19 (but not who were reported as “Long COVID”) found that:
- There were two clusters of enduring symptoms: one that involved physical health, the other involving mental health.
- Subjects tested lower than the population average on processing speed, reasoning, and verbal processing.
- Subjects did not test lower on memory.
- Cognitive ability correlated with physical symptoms; cognitive ability did not correlate with mental health symptoms.
This study from Ontario covering the first year of the pandemic found that COVID-19 doesn’t stop when you test negative. Women in Ontario who had had COVID-19 an average of almost 2 more health care encounters per person-year than those who did not have COVID-19. Men had 0.66 more health care encounters per person-year.
This article says that they have pretty strong evidence that the (a?) problem in Long COVID is microclots.
Vaccines
This preprint from the USA found that taking non-steroidal anti-inflammatories shortly after getting a vaccination (to reduce the pain) did not reduce the effectiveness of the vaccine.
This paper shows that antibodies in nasal swabs are much higher in people who have been vaccinated and infected (left, purple bars) than in people who were only vaccinated (right, orange bars):

This is why we need mucosal vaccines!
Bonus: in this paper, they also found a very potent monoclonal antibody (S2X324) which they say is a good candidate for commercialization.
This paper from Quebec reported the protection given by combinations of infections and vaccinations against a BA.2 infection:
| # doses | previous pre-Omicron infection | previous BA.1 infection |
| 0 | 38% | 72% |
| 1 | 56% | |
| 2 | 69% | 96% |
| 3 | 70% | 96% |
Pathology
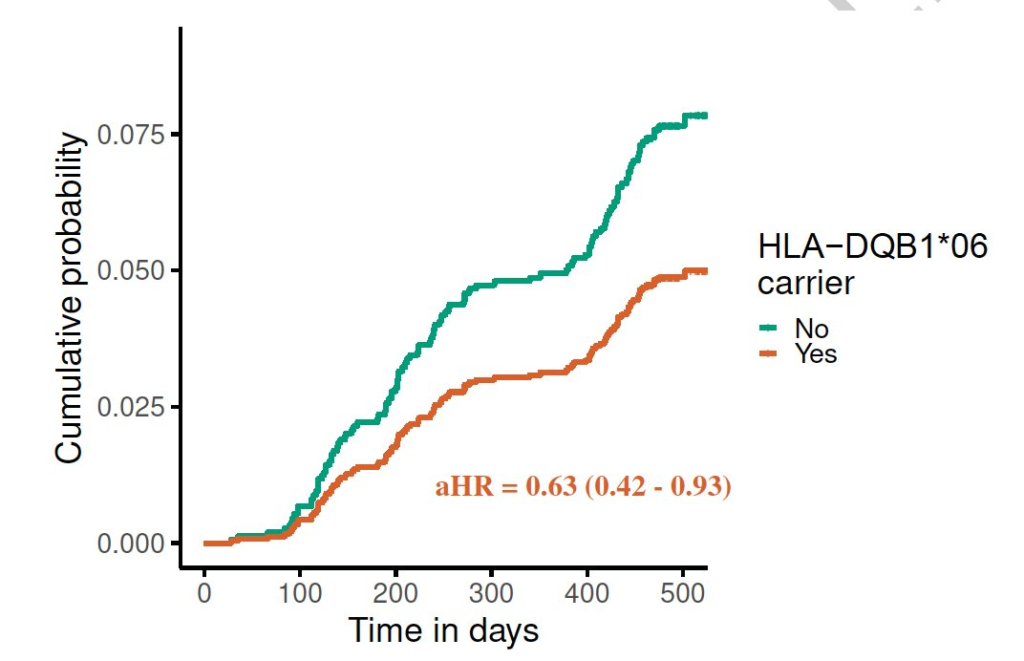
This paper from the UK found a allele which correlates with worse COVID-19 outcomes. Interestingly — and I have no idea what this means — this gene is also associated with narcolepsy.
This article reports on a presentation which found that trauma patients who had asymptomatic COVID had:
- Higher rates of myocardial infarction and cardiac arrest (3.2% vs 0.9%)*
- More ventilator days (3.33 vs 1.49 days)
- Longer stay in the intensive care unit (4.92 vs 3.41 days)
- Longer overall length of stay (11.41 vs 7.24 days)
- Higher hospital charges ($176,505 vs $107,591)
Treatments
This article reports that Health Canada has approved Evusheld as a treatment for COVID-19, available to immunocompromised people over 12. (It was already in use as a prophylactic, similar to a vaccine, as it provides some protection for six months.)
Recommended Reading
This presentation to the US CDC shows that yes, COVID-19 is really bad for pregnant people and infants and that COVID-19 vaccines are not.
This article talks about the promise and danger of “gain-of-function” research.