
COVID-19/MERS
Long COVID
⭐ ❗❗This paper from Japan (2024-12-02) reported that oral minocycline significantly helped 89% of long COVID patients in what was effectively a big case study, especially when given in the first six months. There was improvement in fatigue, post-exertional malaise, unrefreshing sleep, brain fog, disequilibrium, orthostatic intolerance, and neuropathic pain. (Minocycline is an antibiotic, but also has a number of protective effects on neurons.)
This was actually an ME/CFS study, with 55 total patients, 19 of which were Long COVID patients (though one dropped out due to side effects). 89% of the Long COVID patients who stayed with minocycline were helped, while (if I did the math right), only 75% of the non-Long COVID patients were helped.

Oral minocycline does frequently give unpleasant levels of nausea and/or dizziness, so it’s not an ideal medicine. Also please note that
- Not everyone was helped;
- People who had ME/CFS for longer were helped less;
- This was not a randomized trial — there was no control group, so partly this might be placebo effect.
- These weren’t the sickest Long COVID patients: people had to be able to stand and walk (and, it appears, to come to a hospital) in order to participate in the study.
- Most of the improvement was in people who had Long COVID for less than six months, so maybe they would have recovered on their own.
However, it is encouraging news!
This paper from Simon Fraser (2024-12-06) reports survey results that Long COVID impacts people’s lives (duh), but does so unequally. For example, older long haulers had decreased mobility and increased pain, but younger people had more anxiety and depression.
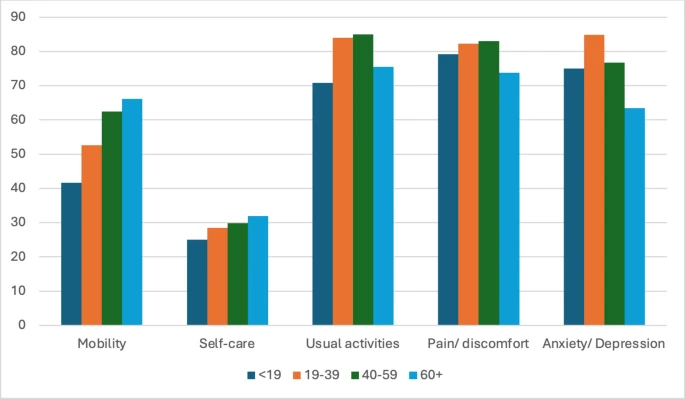
They quantified different symptom rates:
- 82% reported difficulty doing usual activities (i.e. work, study, housework, family, or leisure activities);
- 81% reported some pain/discomfort;
- 76% reported mental health problems;
- 60% reported problems walking around;
- the majority were able to dress and wash themselves;
- 16% “lost their job due to COVID-19” (but it doesn’t say if it is due to Long COVID or because they e.g. got laid off due to lack of work);
- 5% reported no impact from Long COVID. (Do they have Long COVID if they have no problems??)
Being a visible minority, living alone, being unemployed, being older, being female, and especially being unable to work unsurprisingly correlates with suckiness in most dimensions more than the reverse conditions.
⭐ The paper mentioned this study from StatCan (2023-08-23) that BC has 65,000 adult long haulers — which works out to 1.4% of the BC adult population. 82% of 1.4% means 1.1% of the adults in BC has difficulty doing usual activities. 😬
The WorkSafeBC COVID-19 claims site says that WorkSafeBC has only allowed 18,423 COVID claims to date. That’s 28% of the number of long haulers, and I honestly can’t decide if that’s good or bad. The site notes that workers have to prove their risk of contracting the disease in the workplace was significantly higher than the risk to the public at large, and their approval rate is 87%.
⭐ This paper from UK (2024-12-02) has good news and bad news. The good news is that ~70% of children and young people who had Long COVID three months after their acute stage recovered by 12 months! The bad news is that 30% did not.
Interestingly, vaccination made no difference to Long COVID recovery. Maybe vaccination helps you avoid Long COVID but if you get it, ya got it as bad as anyone.
This paper from Spain (2024-11-27) reports that there is a slight increase in the risk of persistent Long COVID with higher levels of particulate matter. They also noted that unvaccinated people had about a 3x risk of Long COVID compared to vaccinated people.
Mitigation Measures
⭐ This article from USA (2024-12-05) mentions that nearly 75% of restaurant meals are now consumed off-premises, up from 60% pre-pandemic. I was surprised at how high numbers were, even in the Before Times — maybe that figures include coffee and doughnuts?
⭐ This study (2024-11-29) looked at the difference between everybody wearing a medical mask (“baggy blue”) and everybody wearing an N95-class respirator for ten weeks in hospitals in four countries. They found that compared to the respirator group, the baggy blue group was:
- 2.83 times more likely to catch COVID-19 in Canada;
- 1.54 times more likely to catch COVID-19 in Israel;
- 1.50 times more likely to catch COVID-19 in Pakistan;
- 0.95 times more likely to catch COVID-19 in Egypt.
Overall, the baggy blues group was 1.14 times more likely to catch COVID-19 than the respirator group, but that was mostly because there were a lot more people in the study in Egypt and the Egyptian health care workers caught COVID-19 at basically the same rate regardless of mask. (Maybe they usually caught COVID-19 outside of work? Maybe they didn’t actually wear their masks/respirators in Egypt?)
⭐ This paper from USA (2024-11-27) reports that in ten hospitals, masking worked. The ratio of patient hospital-acquired infections (i.e. 4 days or more after admittance) divided by patient community-acquired infections (i.e. before 4 days post-admittance) increased by 25% when universal masking was dropped, then fell by 33% when masking for the health care workers only at the hospitals resumed.
Pathology
This article from New York City (2024-11-29) reports that new drivers in NYC have been flunking their drivers’ tests at higher and higher rates since COVID appeared. Nearly half (48%) are now flunking their first try, vs. 41% pre-pandemic.
Now, this might be other factors. Maybe a lot of the new drivers are Venezuelan asylum-seekers, and Venezuelans are crappy drivers? However, there have been other studies about COVID-19 degrading cognitive abilities (see this article from USA (2024-11-16), even about how COVID-19 affects driving. I also remind you of this paper from USA (2024-10-08) which correlated auto accidents with COVID-19 infection rates and concludes that the risk of car crashes “associated with” COVID-19 is comparable to the risk of driving drunk. (NB: I don’t know what “associated with” means, and the full paper isn’t out yet. I have asked one of the authors for a copy.)
⭐ This paper from Sweden (2024-11-29) reports that getting COVID more than doubles the risk of getting Multiple Sclerosis and other conditions that damage nerves’ myelin sheaths.
⭐ This paper from Canada (2024-12-06) reports that patients with influenza A, influenza B, or RSV are more likely to get a bacterial infection than COVID-19 patients. Compared to COVID-19 patients, patients with:
- influenza B are 2.3 times as likely to get a bacterial infection;
- influenza A, 1.69 times;
- RSV, 1.56 times.
This paper (2024-12-03) reports that COVID-19 can damage the retina cells of mice.
⭐ This article (2024-11-15) about this paper using data from the USA (2024-11-15) reports that the number of babies born with heart defects in the first year of the pandemic was 16% higher than pre-pandemic.
Vaccines
This paper from Switzerland (2024-11-30) reports that some people get chronic uticaria (hives) shortly after getting a COVID-19 vaccine, especially Moderna’s Spikevax. (Unfortunately, the paper didn’t say how common it was.) They also found that 100% of a small sample (four out of four) of people who developed chronic uticaria after a vax were able to tolerate another shot of Spikevax with no increase in uticaria problems, so it looks like whatever the vax is doing, it’s an indirect effect.
⭐ This outline of the August 2024 Coalition for Epidemic Preparedness Innovations (CEPI) Scientific Advisory Committee (SAC) meeting had a section for “Broadly Protective Coronavirus Vaccine (BPCV) portfolio strategy”, where they talked about pan-Sarbecovirus vaccines. Things I thought were interesting:
- One thing that was clearly important to them was creating, in the language of software development, test cases. CEPI is developing libraries of viruses which vaccine makers can then use to test how good their vaccines are. I have the sense that these would come packaged in a kit that researchers could just order.
- They talked about what the use case for a pan-sarbecovirus would be: would it be for regular use? when there was a pandemic? They recommended that they develop a vax to stockpile for use in case of emergency.
- They noted that pre-clinical (i.e. in animals) studies of a pan-sarbecovirus would be in animals which had never seen SARS-CoV-2 or common cold coronaviruses, while most humans have some experience with coronaviruses. That might reduce the applicability of new vaccines.
- “It was noted that there is not currently a use case for SARS-CoV-2 vaccination in [lower middle income countries (LMICs)]”, they said. Does this mean that they just aren’t going to vaccinate for COVID-19 in LMICs any more??? (I would be even more offended by the idea of just letting LMICs catch COVID-19 over and over if I didn’t see some high income countries also rolling over and playing dead.)
- It might be difficult to get regulatory approval for a pan-sarbecovirus.
- How would you prove that it worked on lots of strains, especially ones which are no longer circulating?
- Regulatory agencies usually want to see justification for every component that goes into a vax; how would you legally justify including a component for a variant which isn’t currently circulating, like MERS?
- Generally to get approval for a new vax, you have to prove “non-inferiority” to a vax which has already been approved. What if you make a vax which works against all of A, B, and C, but it isn’t as good as the W vax against A, the X vax against B, and the Y vax against C? One might hope that since the new vax is good against A, B, and C, it would also be good against D, E, and F which we haven’t seen in humans yet — but how could you prove that?
Testing
I have an independent datapoint on the availability of rapid tests: someone who is not me picked up a box on Friday in Vancouver in the South Granville neighbourhood.
Treatments
⭐ This paper (2024-12-03) which looks at soluable ACE2 levels sent me chasing more information. Apparently, cells can naturally shed things that look just like ACE2 receptors, but they aren’t anchored to the cell. This means that the freefloating (“soluable”) ACE2 thingies act as decoys, so the spike protein can latch harmlessly onto them. I had previously wondered if flooding the body with fake ACE2 would work, but I figured that given that the ACE2 receptors were freakin’ everywhere, they were kind of important for bodily function, and having important bodily molecules also grabbed by the decoys would be harmful.
Well, there has been prior research which seems to indicate that flooding the body with decoy ACE2 is okay:
- This case study (2020-09-24) was saying that soluable ACE2 helped a very sick patient… and apparently her body didn’t mind having all the ACE2 receptors surrounded by decoys.
- This paper (2024-01-23) found that mice given soluable ACE2 and a high dose of Delta had a 90% survival rate, compared to a 0% survival rate for mice given placebo.
- This paper (2023-04-11) reports that giving mice soluable ACE2 intranasally is quite good. Mice were given no treatment, intranasal soluable ACE2 (IN), intraperitoneal soluable ACE2 (IP) before and after infection with a high dose of COVID-19. 90% of the IN group, 40% of the IP group, and 0% of the untreated mice survived. (NB: This paper was done by the same research group as the immediately previous paper.)
Back to the first paper I was talking about (the 2024-12-03) one: they measured soluable ACE2 over time, and found that cells slowly stopped shedding soluable ACE2 for some time after the acute phase. They said that showed that a SARS-CoV-2 “infection” was not a binary thing that stopped after a week or two, but something that gradually went away.
Transmission
⭐ This preprint (2024-12-06) reports that 39% of camels sampled in Saudi Arabia had MERS. I can’t decide if this is bad news (because omg so many camels!) or good news (because it means MERS is probably a lot less lethal or contagious than we thought).
Recommended Reading
If you geek out on COVID-19 vaccine progress, read Hilda Bastian’s latest blog post.
A friend reminded me of this paper from Hong Kong (2004-11-23) about the original SARS-1 outbreak in the Hong Kong Amoy Gardens apartment complex twenty years ago. I had read this paper twenty years ago but forgotten it, and I read it now with great sadness: the paper makes it stunningly obvious that SARS-1 was airborne. TL;DR: People in an apartment tower sixty metres away from the index case got infected.
H5N1
Transmission
⭐ This paper (2024-12-02) reports that ferrets don’t shed bird-strain H5N1 into the air all that well. They did find that ferrets did shed a lot of H1N1 and mammal-strain H5N1 into the air
Vaccines
The CEPI SAC meeting (which I mentioned in the COVID-19 section above) also had a section on H5N1. Things I thought were interesting:
- “Management noted that pandemic influenza is not currently a priority pathogen for CEPI.” I guess this makes sense, as it’s a possible threat, while there are all kinds of pathogens with a clear and present dangers.
- They are looking at how they can make a pan-H5N1 vaccine — which has many of the same challenges as a pan-sarbecovirus has.
- “Ultimately, CEPI should target many shots on goal [in developing a vaccine], not picking a single winner.”
Recommended Reading
⭐ Why have almost all of the bird flu cases been so mild, when “they” were all saying it had a case fatality rate of like 50%?? This article from USA (2024-12-02) discusses that very question. Hypotheses which they look at:
- Maybe infection through the eye isn’t as deadly as when it’s inhaled.
- Maybe the 2.3.4.4b strain isn’t as deadly.
- Maybe we’re getting some protection from having gotten different HxN1 viruses in the past.
- Maybe there were a lot of mild cases which we just never noticed before, which would bring down the case fatality rate.
Mystery in DR Congo
There is some mystery disease that has been killing people in a remote part of the DR Congo. This article (2024-12-05) reports that it appears to be respiratory in nature. It’s in a really remote region, so there aren’t diagnostic testing labs nearby and it’s taking a while to get tests run. It’s quite possible that it’s one of the usual suspects and is just taking a while to find that out.
Recommended Reading
⭐ The mystery outbreak apparently has had really fluctuating numbers reported for both cases and deaths. This blog post (2024-12-05) explains why numbers can change so drastically.