
Long COVID
This paper from USA (2024-07-03) reports that they find SARS-CoV-2 hangs out in the bodies of people who had COVID-19. They’ve got a technique where they do PET scans with a tracer that can show where in the body T cells are active. They see a lot of activation in Long COVID patients where it shouldn’t be; they see a correlation between high activation in the lungs and pulmonary Long COVID issues. They then went and did colorectal biopsies (OW!) and found SARS-CoV-2 in five of five of the biopsies — including three who had had symptoms for over 676 days!
This video (2024-06-24) by one of the people in the study, showing off his tracer PET scans is really interesting — and sobering.
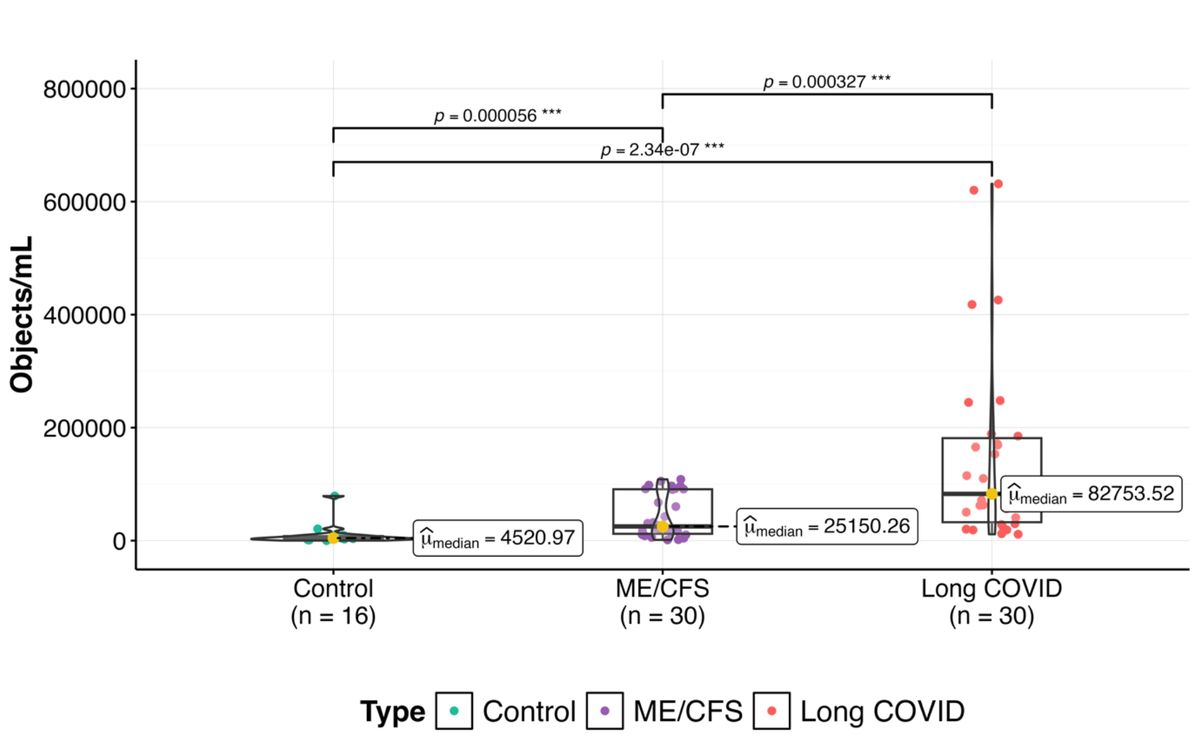
This preprint from South Africa (2024-06-24) reports that microclots are a real thing in Long COVID. They measured the number of microclots in healthy controls, people with ME/CFS, and people with Long COVID. People with Long COVID had more clots that people with ME/CFS, who had more clots than healthy controls:
This paper from Spain (2024-01-04) reports that pregnant women were likely to get Long COVID. They found that 34% of women who had COVID while pregnant between March 9th, 2020 to June 11th, 2022 had at least one post-COVID symptom three months or more after their infection.
However, this paper from USA (2024-01-22) reports that the prevalence was much lower, though partly that might be due to different definitions. They found that 9.8% of people who had COVID-19/Omicron while pregnant had Long COVID after six months.
Vaccines
I have gotten a variety of vaccinations because I have a deep, fundamental belief that diversity is good. Most of the research papers I’ve seen have not backed me up on that: generally, the higher the amount of mRNA, the better the vaccine effectiveness. (*cough* Moderna *cough*). HOWEVER, this paper from Japan and South Korea (2024-06-25) reports that heterogenous vaccination is good! They found that compared to people who never caught COVID-19, there were large increases in risk for new neurological disorders in both the short term (first 30 days after infection) or long-term (after the first thirty days):
| Vax type | before 30 days | after 30 days |
| None | 3.5x | 1.89x |
| mRNAs | 1.39x | 1.24x |
| viral vectors (e.g. AZ) | 1.66x | 1.12x |
| both mRNA and viral vector | 0.61x | 0.66x |
Let me repeat and rephrase because it’s wild: if you got an mRNA vax, a viral vector vax, and then got COVID-19, your risk of getting a neurological disorder is lower than if you had not gotten COVID-19. (They didn’t have a category for “got a vax, didn’t get COVID-19”.)
If you want to see what’s new and shiny in vaccine trials, this blog post is worth reading. Tl;dr: not that much right now.
Okay, now this is just weird: this Research Letter (i.e. not peer-reviewed, I think) from USA (2024-07-03) reports that with each increase of 10 percentage points in COVID-19 vaccination coverage, parent-reported child asthma symptom prevalence decreased by 0.36 percentage points. Asthma reductions didn’t correlate with masking or with COVID-19 infection incidence. Wild.
CREDS (COVID-Related Excess Death and Sickness)
This paper from Japan and South Korea (2024-06-25) (yes, the same paper that was mentioned earlier) reports that COVID makes you more likely to get neurological disorders. People who got COVID-19 were 2.35 times as likely to get a new neurological disorder diagnosis in the 30 days after getting COVID-19 than people who did not get COVID-19.) People who got COVID-19 were also 1.36 times more likely than people who had a non-COVID-19 acute respiratory illness to get a new neurological disorder in the 30 days after infection.) Some of the increased risks were huuuuge: people were 12.34 times more likely to get encephalitis and 11.89 times more likely to get Guillain-Barré syndrome than controls.
They found that people who had mild COVID-19 cases were “only” twice as likely as controls to get a new neurological diagnosis, while people with moderate-to-severe (which I suspect is code for “hospitalized”) COVID-19 cases were 4.18 times as likely to get a new neurological diagnosis.
The risk dropped over time for the first six months, but was still a bit elevated at the one-year mark.
This paper from Italy (2024-03-19) reports that people who had COVID-19 are 73% more likely to have major cardiovascular events. The risk was highest in the first year, but stayed above the COVID-free patients for at least three years.

This Original Investigation (which might mean “unreviewed) from Finland (2024-06-27) reports that ADHD diagnoses went up by 18.60% since the start of the pandemic, with some subgroups having almost a 3x increase.
Pathology
This paper from Finland (2024-07-02) reports that living (well, as much as viruses “live”) SARS-CoV-2 persists even in corpses. In an autopsy study, they found culturable SARS-CoV-2 virus in skull sawdust in 4.5% of COVID-19 patients. (The study didn’t say if the patients died of COVID-19 or if they had Long COVID, or how long before death they tested positive. They were looking at it from the standpoint of “what is the risk to pathologists?”)
Recommended Reading
This blog post talks about mask bans, and goes into some detail into the economic reasons why politicians might be against masks. Tl;dr: masks are a danger signal, and people spend less money when they are reminded of danger.
Here’s another article that you can give to people who wonder why you are still COVID-cautious. (But they probably won’t read this one, either.)
Treatments
This paper from China (2024-05-28) reports that olgotrelvir reduces COVID-19 recovery time by 22%.
H5N1
Transmission
This press release (2024-07-01) from US CDC says that a fourth human, in Colorado, has tested positive for H5N1.
This article (2024-07-02) reports that fully a quarter of Colorado’s dairy herds — all in the northeastern corner of the state — have had H5N1 outbreaks. What’s worse, several of the herds were “closed”, meaning that no cows from outside came in. That means that it spread by some other vector. The article doesn’t mention birds as a possible vector, because if it was that easy to catch it from birds, all the herds would be infected. That means it is likely that humans are carrying it with them somehow — either in their bodies or on objects they move around from herd to herd. (Maybe it was the person who tested positive in Colorado (above)?)
This article says that there are now 137 cattle herds infected with H5N1.
It also reports that there have been a few detections of H5N1 in San Francisco (which is not known for dairy cows!). They are guessing that maybe it came from live-bird markets.
Vaccines
This press release from Moderna says that they got $176 million of funding from the US Government to develop an mRNA bird flu vaccine. They said that they’d already started a Phase 1/Phase 2 clinical trial, which they expect to be done before the end of 2024.
Recommended Reading
If you want to get depressed about how the US is bungling bird-cow flu, read this article (2024-06-18) about what a good job Finland did when they found bird flu in minks.