
I’m going to split blog postings into COVID-19 sections and H5N1 sections for now. I might someday split them into separate postings.
Psychology
Many years ago, I heard this George Carlin joke: “Have you ever noticed that anybody driving slower than you is an idiot, and anyone going faster than you is a maniac?” It sort of makes sense: anybody who is not going the exact same speed as you has a different relative speed, and as such they are a bit of a threat. Drivers going faster than you are more dangerous than slower ones (because you do not have eyes in the back of your head), but even the slower ones are a bit of a danger to you if you hit them. Slower drivers also reduce your enjoyment of life, in making you wait longer before you get to the thing you want to do.
I realized that the same thing is happening with COVID-19. Carlin today might say, “Anyone who is being less cautious than you is a maniac, and anyone who is being more cautious is over-reacting.” If you interact with someone who is less cautious, you will find their behaviour dangerous to you. If you interact with someone who is more cautious, they will be no fun. 🙁
Meanwhile, everybody is mad at the people responsible for involved public health, including public health organizations, but also “the government” and scientists. On one end of the scale, the COVID deniers are mad that there were any mitigation measures at all, while on the other end, the COVID-cautious are mad that mitigation measures have been abandoned. In the middle, there are people who are okay with some aspect(s) of the mitigation measures, but are mad about some other aspect(s). It’s pretty fucked up, but I guess I shouldn’t be surprised that, y’know, a global pandemic would cause lasting damage to society. 🙁
COVID-19
Long COVID
This paper from USA (2024-04-26) found that people who got a booster were 25% less likely to get Long COVID than people who were unvaccinated. (The paper is paywalled, so I couldn’t see what the relative protection was between boosted and vaxxed-but-not-boosted was, and I didn’t think it was important enough to call in a favour to get the article.)
This paper from Australia (2024-04-17) found that 62% of people with Long COVID were better after two years. Another way of looking at it, however, is that 38% weren’t any better after two years.
This paper from USA (2024-04-21) found that 48.5% of long haulers eventually recovered. However, those with severe COVID-19 symptoms and those who had more than a high school degree, were aged 40 years or older, or were female were less likely to report recovery. Latinx adults were significantly more likely than Whites to recover.
This preprint from USA (2024-05-01) found that 51.2% of long haulers at a specific clinic felt they got better after at least a year. Again, that means that about half did not get better.
A few weeks ago, I talked in my General blog post (2024-03-22) about how SARS-CoV-2 infects bone marrow megakaryocytes, which causes the immune system to freak out and go nuclear, causing clots among other things. Well, this conference presentation from France (2024-03-03) reports that they found higher levels of megakaryocytes infection in Long COVID patients than healthy controls, platelet microclots in all of their Long COVID patients, and spike in 30% of Long COVID patients’ blood plasma (and 0% of controls). I have a real sense that megakaryocyte infection is important.
This paper from BC using data from USA (2024-04-25) found that people with Long COVID had various psychiatric disorders (anxiety, sleep difficulties, cognitive difficulties) at about twice the rate of non-long haulers, and had about 85% higher risk of disabling fatigue.
This paper from Serbia (2024-04-30) found that a creatine-glucose supplement for eight weeks decreased several symptoms in long haulers.
Vaccines
This press release from the World Health Organization says that the next boosters should be from “a monovalent JN.1 lineage”. Note that they didn’t that it should be exactly JN.1, but from JN.1 or one of its descendants. This gives some wiggle room, which is good because it looks like JN.1 and KP.2 are pretty different. (This preprint suggests that the current booster (XBB 1.5) won’t give much protection against the next strain on the horizon (KP.2). Previous papers said that XBB 1.5 worked pretty well against JN.1, ergo KP.2 is different from JN.1.)
This paper from Korea (2024-04-25) says that for people who had a prior uveitis infection, getting a COVID vaccination gave them 51% to 107% greater chance of getting a re-infection, depending on which vaccine they got.
Pathology
This paper from BC (yay BC!) (2024-04-24) found that people who had a positive COVID-19 test in 2020-2021 were at higher risk of a heart attack in the following months (average followup time of 260 days) compared to controls:
- all COVID-19 cases: 1.34x risk;
- hospitalized cases: 3.81x risk;
- ICU cases: 6.25x risk.
They estimated that COVID-19 has made the rate of heart attacks in BC ~7% higher.
This paper from USA (2023-12-14) found that people hospitalized with COVID-19 in the first ~two years of the pandemic were 51% more likely to die in following the 18 months than people who were hospitalized with influenza in the ~four years before the pandemic. COVID-19 is not the flu!
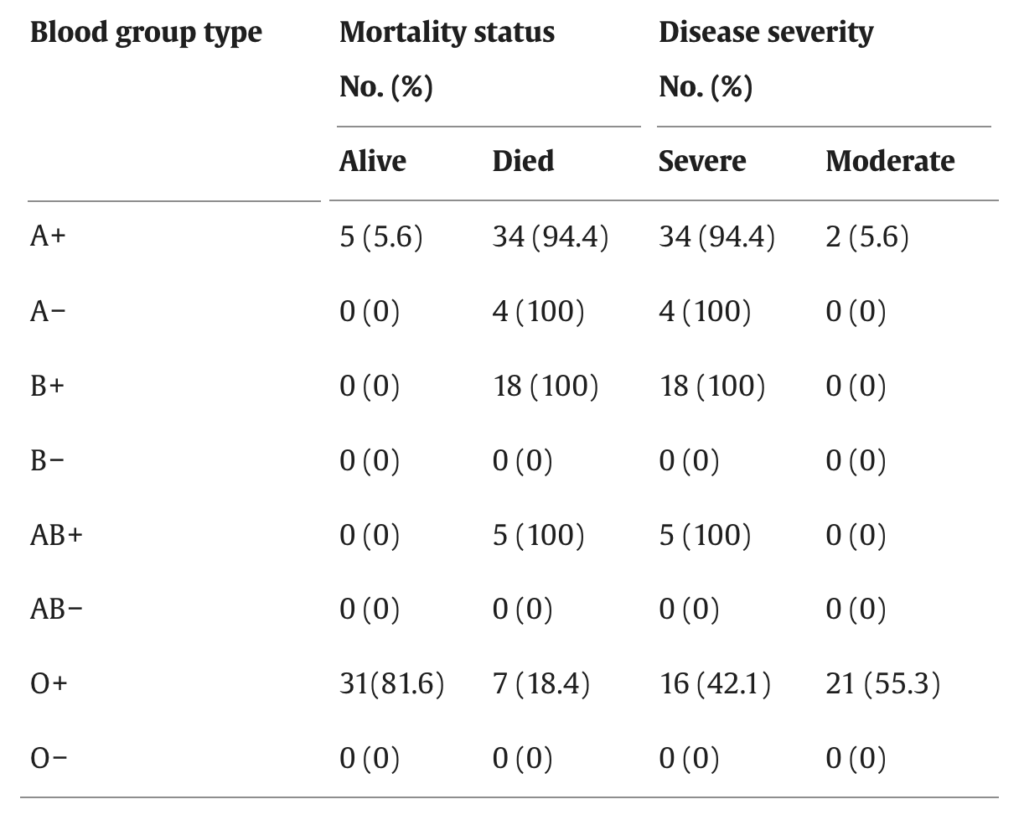
This paper from Iran (2024-04-13) found that people hospitalized for COVID-19 in 2021 who had O+ blood were unlikely to die compared to other blood groups. All of the A-, B+, and AB+ patients died, and most of the A+ patients died. They didn’t have any B-, AB-, or O- patients, but didn’t talk about whether that was because there just aren’t many people with that blood type or if those blood types didn’t get hospitalized.
This old paper from Iran (2022-10-25) found that erectile function in men with moderate or even mild COVID-19 cases was statistically significantly worse than in controls. Men, avoid COVID-19 to protect your sex life!
Treatments
This paper from UK (2023-12-22) found that Molnupiravir wasn’t any better than standard care without Molnupiravir.
Last week, I talked about how the antibiotic neomycin strongly protected mice against COVID-19. Neomycin happened to come up at a doctor’s appointment, and the doc told me NOT to use neomycin, that it was evil, because it promoted allergies. Maybe neomycin boosts the innate immune system because of its allergenic properties, not its antibiotic properties.
This paper from USA (2024-01-31) found that hot commercial black tea reduced COVID-19 loads in the mouth by 68% to 90%.
This paper from USA (2024-05-01) found that people who took metformin were 28% less likely to have detectable viral load than placebo at day 5 or 10, and 32% less likely to have viral rebound than people who took a placebo.
The above paper also looked at ivermectin and fluvoxamine, and found they had no effect. (Why is anyone still looking at ivermectin? Because the trial started on January 1, 2021 and ended February 14, 2022. Papers take a long time to get published.)
This paper from USA (2024-04-25) found that patients hospitalized with COVID-19 who took abatacept (most commonly used as an arthritis drug) had a 48% lower chance of dying. It is a rather expensive drug, unfortunately.
Transmission
This paper from UK (2024-05-01) and (this mass-media article) reported on a 2022 COVID-19 challenge study of people who had been previously infected. (A challenge study is one where they deliberately infect people.) They had a problem: nobody got sick! They used a dose of COVID Classic that had gotten 50% of the COVID-naive (never vaccinated, never infected)participants sick in a previous study, and when that didn’t work, they kept boosting the dose. They increased it to 10,000 times what the first study had used, and still couldn’t get anybody sick.
This would be really encouraging, except for the fact that 40% of the participants got Omicron infections afterwards. 🙁
(Also note that the participants of both studies were selected to be young and healthy, to minimize the danger of the study.)
Testing
This report from USA (2024-04-24) found that rapid tests were only about 47% effective (when compared to PCR tests) in the study period of November 2022 to May 2023.
They also found that the peak positivity was three days after symptom onset.
Recommended Reading
If you are a vax nerd, this newsletter has all the latest news. TL;DR: there are some promising developments, but nothing that is very close to going into production.
H5N1
DO NOT DRINK RAW MILK! (See below under Transmission.)
Having said that, I do not think a A/H5N1 2.3.4.4b (avian-bovine flu) pandemic is a danger to you right now (if you don’t eat raw milk). It certainly could happen, but I don’t think it is happening yet. Yes, H5N1 has jumped to humans, but:
- The symptoms that the infected humans (that we know about) are not terribly scary; none have died that we know of.
- Various article (including this one) report that the FDA has tested milk and found that pasteurization kills H5N1.
- The US already does a lot of influenza surveillance, and despite the bovine H5N1 having been around since last fall, the US flu season has looked bog standard. It started at a normal-looking time, the levels were normal-looking, there weren’t any funny spikes. (I have been looking at flu stats every week during the flu season for several years.)
- The US surveillance does genotyping on a subset of its flu, including sorting it into H1Nx, H3Nx, and “other”. If it was getting an unusual number of “others”, I think they would have noticed.
- They haven’t found human-to-human transmission (yet), although to be fair, US CDC is encountering some difficulties in their contact tracing. (Dairy farmers frequently employ undocumented workers, so are not always really excited about letting government agents poke around, and the workers themselves are resistant to being interviewed. Yet another reason why being hostile to immigration is a Bad Thing!)
So I don’t think that bovine H5N1 transmission is not particularly nasty, and it doesn’t look like human-to-human spread is easy. This certainly doesn’t look like something comparable to COVID-19. Yet.
Could it become nasty and/or contagious. Absolutely! There is a genuine danger of that, and it could be far worse than COVID-19. But as far as I can tell, it hasn’t happened yet.
Vaccines
We are, in some ways, better prepared for H5N1 than we were for COVID-19, especially regarding vaccines. If there is a nasty outbreak, we will get vax pretty fast.
- There are already vaccines approved for use against H5N1. We can go straight to production without waiting for three rounds of clinical trials to finish.
- The US (which is where the bovine H5N1 has been found) already has a stockpile of ~5M treatments worth of H5N1 vaccines. Not enough to vaccinate everybody, obviously, but enough to get a really solid jump on vaccinating health care workers, dairy workers, etc. Canada apparently does not have H5N1 vax in stockpiles yet, but this article says they are thinking about it.
- We humans know how to make flu vax, we’ve been doing it for decades. The way that flu vax has traditionally been made (incubating in eggs) is slow, but highly predictable (and cheap).
- There are several mRNA flu vaccines (which can be made much faster than the other vaccines) well along the pipeline. According to this press release, Pfizer started a Phase 3 trial for an mRNA influenza vaccine in September 2022. This press release says that Moderna started a Phase 3 trial of one in June 2022. Yes, both of those are for “normal” human influenza, but influenza vax is kind of special because they have been making it for years and it changes every year. According to this Government of Canada web site, once a company gets their influenza vax approved once, then all they have to do to make flu vax with different strains is file update paperwork, but they do not have to do clinical trials all over again. Maybe that’s for “normal” H1 and H3 strains, but maybe they’d let an H5 through without clinical trials.
- The US approval process is similar to the Canadian process in not needing clinical approval to change the strain of an already-approved vax (read about the process in great detail here). Additionally, they have an accelerated approval path for brand-new vaccines (not just new strains) “when the supply of influenza vaccine is insufficient”, and can then use the hemagglutination inhibition (HI) antibody response as an indicator of effectiveness instead of having to wait for their trial subjects to get sick.
- Moderna started a H5N1-specific vax (not just “general flu”) Phase 1 clinical trial in July 2023, so even if Canada won’t let H5N1 through with just an update, they ought to be able to get approval for their H5N1 vax soon.
- If we do get an H5N1 pandemic, vaccine trials will go faster: it’s easier to study how well a vaccine works if you have lots of sickness.
- There are various universal flu vaccines in the pipleline, including this universal “regular human” flu (A/H1, A/H3, and B) vaccine which should be done with Phase 1 by now.
- This paper (2022-11-24) describes a flu vax which works against ALL known influenza strains (yes, including “animal” strains), but it’s farther down the pipeline. I sent email to one of the authors, who said that they are planning on Phase 1 trials at the beginning of next year (but didn’t say with which partner, if anybody, and I politely didn’t ask).
- Other companies are working on mRNA flu vaccines, some of them targeting H5N1. This press release says that CureVac has finished Phase 1/2 trials of its mRNA seasonal (i.e. H1/H3/B) flu vax. This press release says that Sanofi started a seasonal mRNA influenza trial in June 2021, but I don’t know how that went (but I didn’t try very hard to find out).
For more on how fast we humans could ramp up H5N1 vaccine production, see this article.
Treatments
We know how to treat serious influenza. In particular, Tamiflu is believed to work against H5N1.
Transmission
DO NOT DRINK RAW MILK RIGHT NOW. This report from US CDC says that about half of barn cats that ate milk from diseased cows at one farm died.
Should you drink regular milk? Given that we haven’t heard of massive numbers of Americans getting sick, I think it’s a pretty reasonable bet that pasteurization does kill viruses like, y’know, it is supposed to. I am still drinking milk.
What about cheese? I believe that the chances of pathogens surviving in hard cheeses is very very low. The chances of pathogens living in soft cheeses made with pasteurized milk is lower than in pasteurized milk itself, so I think also low. The chances of soft cheese made with raw milk? Then you start getting into a scary area. Me, I wouldn’t eat soft cheese made with raw milk right now (but to be fair, that’s not something I do often anyway).
Is bovine-avian H5N1 even in Canada yet? We don’t know, but it’s pretty widespread in the US (and probably appeared in fall 2023) and as far as I can tell, Canada isn’t even looking for it. Now, while it is true that far far fewer cows fly into Canada to visit relatives than humans do, I expect that there is a fair amount of cross-border cow movement. This page says that breeding cows coming into Canada have to get checked out by a vet, while cows that are turning into meat right away do not need checks. (Yes, that’s slightly scary, but hamburger that was slaughtered here probably isn’t any scarier than hamburger slaughtered in the US.)
This article says that 36 herds have been found to be affected in nine different US states.
This article and this article and others I have read (but didn’t make notes of because I hadn’t yet decided I was going to include H5N1 in these blog posts) point to avian-bovine H5N1’s likely transmission path being, not through the air, but through the udders. If a milking machine is not perfectly sterilized between cows (and it apparently is hard to perfectly sterilize), then it looks like the second cow could get infected by the first cow’s (obviously unpasteurized) milk.
Pathology
While the case fatality rate for H5N1 in humans is frequently quoted as 50%,