
You might have noticed that I now frequently put the country where the research was carried out next to the link. I do think because different countries have different demographic profiles, different vaccination programs/history, different wave histories, etc. Sometimes this matters, and I am not clever enough to figure out when. If work is done in lab animals or simulations, I don’t bother. I figure lab rats and computers are pretty much the same everywhere.
Vaccines
A reminder that I keep track of vaccine effectiveness here.
I was looking at a study today which said that the vaccine effectiveness for four shots (of whatever they got in the USA, which will mostly be mRNAs) was only 66%. I thought that was depressingly low. HOWEVER, somewhere else (I forget, sorry) made me realize/remember that the vaccine effectiveness is calculated compared to the unvaccinated… and in many places (especially the USA!), the unvaccinated are more likely than not to have gotten an infection. That will push the vaccine effectiveness down, even if the protection a vaccine gives never changes.
—
This paper from Hong Kong looks at Pfizer and Coronavac vaccine effectiveness in the Omicron time period. This is really interesting because they had almost no COVID-19 before then, and they had lots of unvaccinated people. That means their vaccine effectiveness numbers are probably more correct than those from e.g. the USA.
They have data sliced every which way, but it’s good. Some highlights of the Pfizer data:
- For those under 60, effectiveness against mild to moderate disease was 35·1% with two doses and 73·5% with three doses.
- The effectiveness of two doses against severe or fatal disease was between 86·9% for >80 year-olds and 96·3% for 20-60 year olds. For three doses, it was between 98·6% and 99·0%.
- The effectiveness of two doses against death was between 90·3% (for >80 y/os) and 96·8%. For three doses, it was between 97·5% for >80 y/os and 99·2%.
—
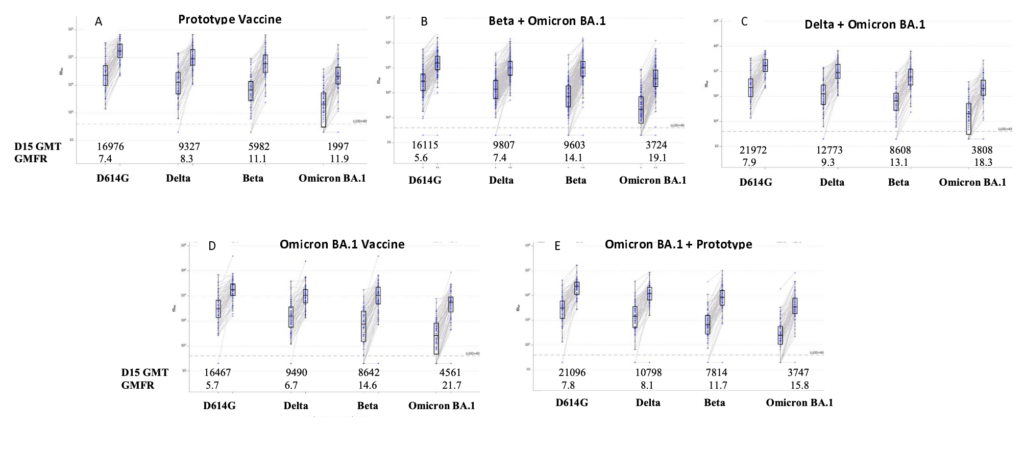
This preprint from the USA says that the various flavours of BA.1-based Moderna vax are better than COVID Classic-based Moderna vax… but not by all THAT much.
This paper (2022-07-19) says many things about many combinations of vaxes and boosters. One thing that makes me happy is that two doses of Novavax plus an mRNA booster works well. (I have two mRNA doses and a Novavax booster, and this is probably as close as I am going to come to seeing data for me.)

This paper from a big study in Hungary found that people who had gotten a second booster were 93% less likely to die from COVID-19 than those who got only one booster.
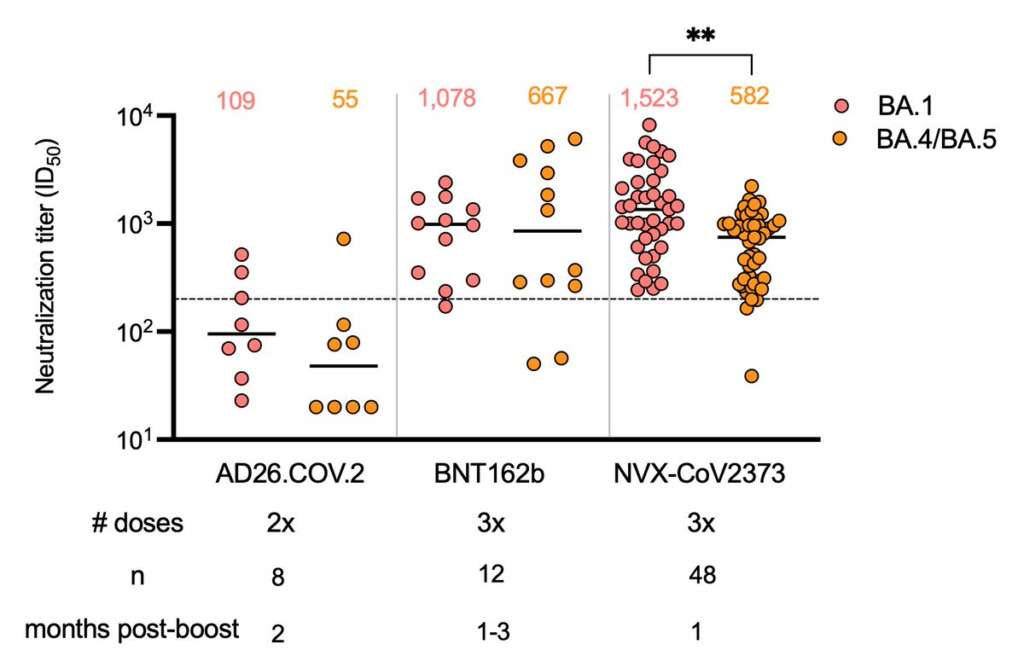
This preprint from South Africa says that three doses of Novavax gave results which were comprable to three doses of mRNA against BA.1 and BA.4/5:
This very confusing preprint from Denmark found that:
- Three doses of vax plus an omicron infection had a vaccine effectiveness of 95% against infection (compared to unvaccinated).
- Vaccine effectiveness was similar for BA.2 and BA.5.
- BA.5 was 65% more likely to send you to the hospital when adjusted by age and calendar period.
Treatments
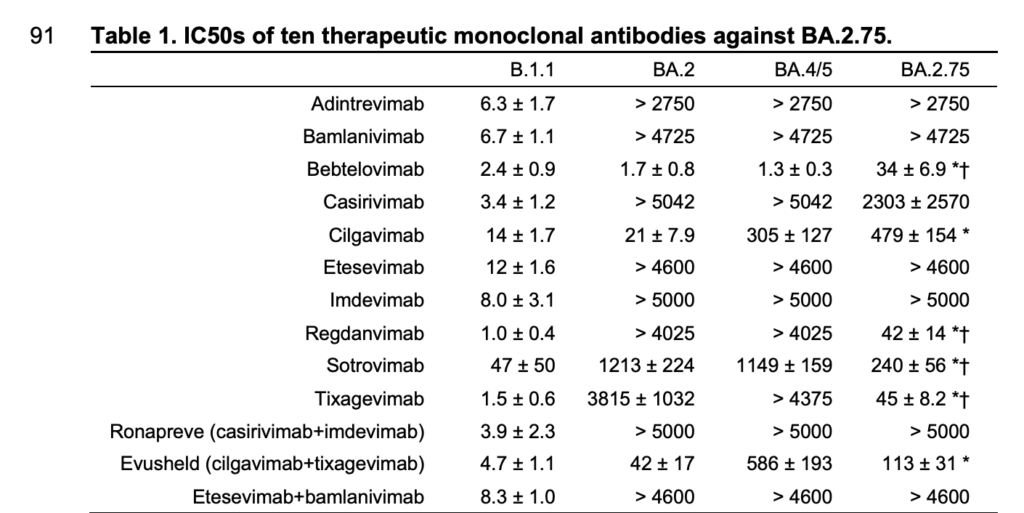
This preprint from Japan says that most monoclonal antibodies don’t work well against BA.4/5. Really only Babtelovimab works well. The good news is that many of them work against BA.2.75, which might be the next variant to take over after BA.5:
This correspondence from Japan and the US reported similar results against BA.4/5 (although they saw some effect of Imdevimab), and also found that all the Omicron variants were about equally susceptible to three antivirals:

Pathology
This article reports on this paper from France that SARS-CoV-2 infected cells can reach hollow tentacles out to other cells — even ones without ACE2 receptors — and shove viruses down those tubes to infect the other cells. Ewww.

This paper from the USA found a genetic marker for increased risk of hospitalization. In addition to maybe being useful for screening, it might also give an clues to better COVID-19 treatments.
This paper says that you’ve got almost a ~5.8x risk of cardiovascular disease (~11.5x times higher risk of pulmonary embolism, a ~6.5x higher risk of atrial arrythmias, and ~5.5x higher risk of venous thromboses) in the four weeks after COVID-19 onset. That drops to ~1.5x in weeks 5 to 12, and decreases farther from weeks 13 to 52.
The paper also says you’ve got an 80% higher risk of diabetes for the first four weeks after you get COVID-19. It drops to 27% higher from weeks 5 to 12, at which point the risk is basically no higher than baseline.
Long COVID
According to this report from the UK, between 4 and 5% of triple-vaxxed adults who got Delta, BA.1, or BA.2 self-report as having Long COVID.
This paper from the US says that the levels of anti-nucleotide IgG antibodies at time of infection predicted well how long it took for patients to clear COVID symptoms. “COVID-19 disease severity, ethnicity, age, sex, and remdesivir use did not affect time to sustained symptom resolution.”
Mitigation Measures
From this tweet (not sure where the data came from), talking about how mitigation measures actually work:

This report says that:
- support for vax passports has dropped from 70% to 25%;
- 74% believe that masks work;
- 51% would support a mask mandate — 55% of in BC and Ontario, 62% in Atlantic Canada, but only 36% in Alberta and 38% in Saskatchewan;
- one third of men under would support a mask mandate, compared to a majority of every other combo of age and gender.
Variants
This preprint says that BA.2.75 is no more immune evasive than BA.5. That’s good to hear (although that’s only one paper, don’t go betting your life’s savings on it).