Press Briefing
IMHO, this was the least interesting press briefing that we’ve had.
Dr.H gave provisional stats, then didn’t really say much aside from telling people that things sucked in hospitals now and exhorting people to Do The Things: stay away from people, mask up, don’t travel, register to get vaccinated, etc.
Surgeries postponed
Dix discussed what the hospitals are doing. The highlight is that they are postponing scheduled surgeries in some LM hospitals for two weeks. This will affect about 750 surgeries in Fraser Health at:
- Surrey Memorial Hospital
- Royal Columbian Hospital
- Abbotsford General Hospital
- Burnaby
It will affect about 1000 surgeries in VCH at:
- Vancouver General Hospital
- Lions Gate Hospital
- Richmond
- St. Paul’s
- UBC
Dix bent over backwards to assure people who got surgeries postponed that he knew that all surgeries are important and that they will get their surgeries. He said that you could trust him on that because that’s what they did last time they cancelled surgeries.
Clinically extremely vulnerable
He mentioned that 224K of the 263K (85%) clinically extremely vulnerable (himself included — he’s diabetic) have gotten vaccinated.
Northern Health
Dix acknowledged the great work they’ve been doing in Northern Health, where UNBC is starting to do surgeries again. I have no idea what that was about, and couldn’t find any news articles about trouble up there.
He also reiterated that they are doing one of the special mass vax AZ clinics in Dawson Creek.
Minister Dix and Dr. Henry both expressed gratitude to Alaska Governor Dunleavy, who is in the Hyder-Stewart area today giving vax. (Hyder is in Alaska but has no roads to the US; they have to get everything through Stewart, BC. People from Hyder are allowed to go to Stewart but only for essential purposes.) I couldn’t find any articles saying so, but Henry/Dix sure implied that Alaska was vaccinating people from Stewart.
Questions
Reminder: I paraphrase heavily and snarkily.
Q: How did B.1.617 get here? A: As you know, we watch variants carefully, and we’ve been watching that one for a while. We’ve seen it in about 40 people in the past two months. Some were related to travel from India, some were not traceable to travel. Note that it is a variant of interest, not a variant of concern. And this is why I am not a high-ranking public official: I would have said, “From people. Next question.”
Q: New modelling from SFU says that herd immunity is a ways off, especially since we are not vaccinating kids. Any thoughts regarding changing the age-priority vaccination schedule? A: I’ve seen that modelling, it’s interesting, but what I took away is that we need high rates across all age groups. And we have seen from Israel, from the UK, that you see a dramatic decrease in cases once you hit 50-60%. NB: I’ve been saying that for a while too.
If you get a high level of immunization so that you get milder cases in younger people, then it’s much easier to handle, even if it doesn’t go away completely. We saw this in Prince Rupert, Cowichan communities, and the DTES when we did mass vaccinations in those places. So for example, the DTES immunizations took a lot of pressure off of St. Paul’s.
Immunization in kids is important. Pfizer is currently licensed down to age 16, and there studies going on now for ages 12-16. We should see results of that study next few months. There are studies which are going down in age to 6 months. I do believe that by next fall, we’ll see vaccines for kids, especially teens. NB: Pfizer finished the study two weeks ago, so I would think it might get approved before school finishes. But I also thought Novovax would be approved by now, so what do I know?
Q: People are saying, “I want to go to my cabin, it’s right across the border” or “I just want to go camping, I promise I won’t talk to anybody”, what do you say? A: Stay local. We have lots of fine places in BC, do it in your home Health Authority. Basically, she refused to be baited into saying, “welllll it’s okay to bend the rules a leeeeeeetle bit…”
Q: We just had a death in a 2 year-old and someone in their twenties, how awful is it going to get in the upcoming weeks? A: We are going to see hospitalizations go up. Fortunately, we have great health care workers go healthcare workers! Honor them by Doing The Things. Oh yeah, we’re going to cut back services.
Q: Is there a way to move staff to hard-hit hospitals? A: What we’re going to do is move patients. For example, patients from the North who would normally get sent to Metro Van will get sent to the Island instead. Usually COVID patients are in hospital longer than they are contagious. After they are not contagious any more, we can move them to one of the non-COVID hospitals.
Q: What message do you have for the public about general hospital use? A: If you are having an emergency, go!! The hospitals are safe, and the ER is there for you.
Q: Couldn’t you give people incentives to get vaccinated by dangling the carrot of allowing them to do some things after vaccination? A: Not yet. There aren’t enough of us vaccinated yet. NB: See my screed in today’s General post. Once there are more of us vaccinated, then we’ll be able to slowly expand what we can do. By the end of the May long weekend, we’ll be in a very different place. NB: I estimate that 63% of BCers will be vaxxed by then.
Q: Grocery store workers are upset that they were on the occupation-track list at first and now they aren’t. A: We had to stop using AZ for reasons outside of our control. We are starting with first responders because that’s what we can do. We have more vax coming, maybe by 1 May, and we will expand the occupation track if/when we get it. NB: BC should get ~36 kilodoses of J&J in the first week of May.
Q: The website says that there’s no airborne transmission, but everybody and their brother is now saying that there is airborne transmission, wtf? A: “Airborne transmission” is a technical term, meaning basically “around corners and through ventilation systems”. Different-sized particles can carry virus, but how well it survives depends upon the size of the particle. It’s not black&white, it’s a gradation. We have always acknowledged that smaller particles can transmit virus, especially indoors, with poor ventilation, unmasked, so absolutely we need to pay attention to indoors spreading and superspreading events. However, we are NOT seeing transmission where there are adequate barriers in place, or people are keeping distance, or wearing masks.
Q: Reports from Ontario are saying that more people are dying at home. Are we seeing that? A: Not that I know of. When someone dies unexpectedly at home, the coroners check for COVID. I don’t think we’ve had an increase in people under monitoring who have died, nor an increase in coroner-investigated deaths which have COVID.
Q: In your modelling presentation, it looked like people were staying in hospital longer. True dat? A: Younger people frequently are in and out in a few days, so our hospitalization duration has actually gone down. But we also have more people who live and thus stay for longer instead of dying quickly. NB: she phrased it much more gently.
Q: When you opened up AZ to the over-40s, suddenly there were massive waitlists. When is Island Health going to get more? Was Island Health’s fair share all redirected to hotspots? A: We have a limited supply of AZ, and mostly we are focused on keeping people out of hospitals, so we targeted those 13 communities. Note that Island Health has very low transmission, thankfully. We are hoping that we’ll get more AZ, maybe we can get some more from the US.
Dix: Note that Island Health has already gotten more than its fair share of vax because most vax has been distributed via the age-based program, and there are a shitton of old folks on the Island. So quit yer bitching. NB: Absolutely not a direct quote. Not even close.
Q: Is all the AZ gone for the over-40s? A: Yes. We gave 180K doses to the pharmacies, and in general it’s in arms or booked to go into a specific arm. There’s 18K headed to the 13 targeted communities, which we expect to use up in the coming week. There is no more AZ on Vancouver Island anywhere.
Q: What about second doses of AZ? A: Don’t fret. We’ve got 16 weeks to figure something out, and they are currently doing mix&match studies happening now. They might say that it’s better to get a second dose of something else. When the studies are done, we’ll be offering options. NB: The way she phrased it, I believe, revealed that she’s pretty sure the studies will say to get Pfizer second. That’s what I’m betting on also.
Q: Some question about hotels that I didn’t understand. A: something which didn’t answer the question in favour of giving more exhortations.
Q: The feds have stopped flights from India and Pakistan, is that too little too late? A: Oh man, things suuuuuuuck in India right now, our hearts go out to them. We fully support the feds in stopping the flights. No, she did not answer the question.
Vaccines
BC has now vaccinated 35% of the adults and 29% of the total population, yay!
We are now vaccinating 11-12 thousand people per day with AstraZeneca vs. more like 6-9K last week.

30 March was when they had to stop using AZ for the occupation-track vaccinations. IMHO, it’s impressive that they got back to almost the same level of vaccinations in just two days (and most of that was on the Easter weekend).
Why were the 40-55 year-olds more excited about the vax than the 55-65 year-olds? I think probably because they knew they would have to wait longer otherwise. When I (in 55-65 cohort) decided to get an AZ shot, I guessed that would only save me three weeks. With my reclusive life, three weeks did not seem like a long time to wait. “Better it should go to someone who needs it sooner” was definitely a thought I had. (I went because I heard that there were slots available, and getting it into my arm meant one more person vaccinated than otherwise.) However, the published schedule shows the 40 year-olds scheduled for vaccination more like six weeks away from now, more than twice as long. NB: I think they are sandbagging. I think it’ll be more like 24 May for the 40+.
We have a bunch of AZ right now, but it’s not clear when we will get any more. Our contracts for AZ vax are with the Serum Institute of India, and India is embargoing vax because of their outbreak (which, to be fair, is probably a better use of the vax than bringing it here). So should those of us who got AZ be worried about a second dose? Nah, they’ll give us Pfizer if there is no AZ, as this article explains.
Courts
A flat-earther (literally) who failed to quarantine and who was thus taken into custody sued the government for kidnapping, terrorism, etc. for that. The court threw out his case, basically for being stupid. Good.
Rapid Testing
There are people who advocate pretty passionately for rapid testing, saying that it would help stop the spread. There are people who argue pretty passionately for asymptomatic testing, and Dr. H keeps saying that they found that asymptomatic testing was not useful — that there were a lot of false positives (because the number of true positives is so low in the general population) and a lot of false negatives (because with a lower viral load, sometimes the virus doesn’t show up). Well, there was just a pilot project at YVR to do rapid testing on departing passengers, and they found zero positive cases. Sounds not very useful to me. 🙁
Statistics
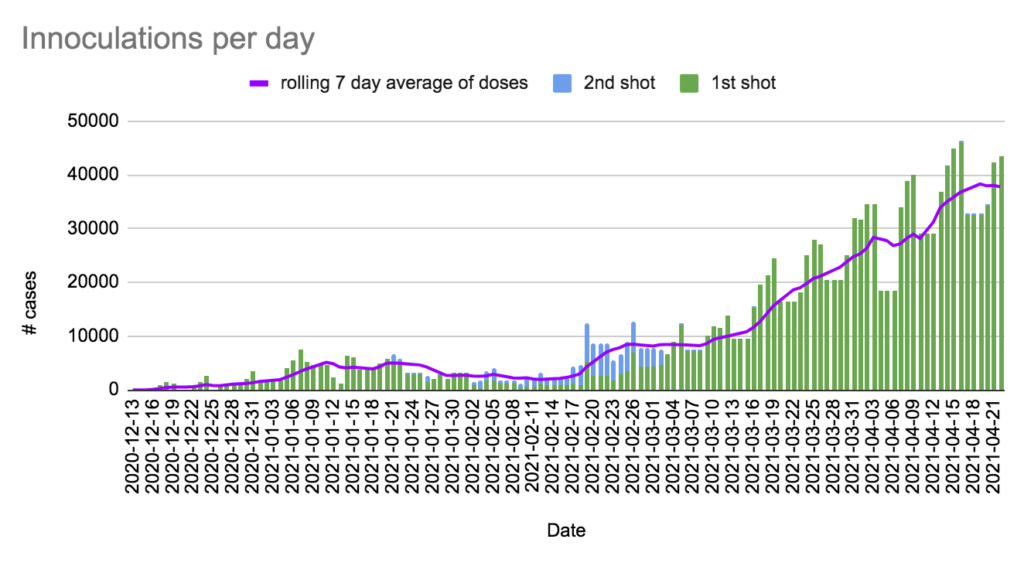
+1006 cases, +4 deaths, +43,474 first doses, +140 second doses (of which 12156 were AZ).
Currently 502 in hospital / 161 in ICU, 8,733 active cases, 12,846 under monitoring, 112,235 recovered.
We have 334,010 doses in the fridges, which we’ll use in 7.7 days at today’s rate. We have given more doses than we had received by 8 days ago.
We have 184,566 doses of mRNA in the fridges, which we’ll use in 5.9 days at today’s rate. We have given more doses than we had received by 7 days ago.
We have 149,444 doses of AZ, which we’ll use in 12.3 days at today’s rate.
Charts