
COVID-19
Long COVID
This paper from USA (2025-06-18) reports that a Delta or pre-Delta infection was protective against further Long COVID, while an Omicron infection was not. People whose first infection was pre-Omicron had about half the chance of getting more than three persistent symptoms after their second infection than after their first. However, people who got an Omicron infection were about 50% more likely to get more than three persistent symptoms after their second infection than after their first.
This paper from USA (2025-06-04) found that patients with the most severe acute COVID-19 infections had the highest risk for new autoimmune diseases. Compared to patients with the least severe acute cases, the patients with the most severe cases had these higher risks, with different risk ratios depending on the cohort that they came from:
- N3C (National COVID Cohort Collaborative) dataset: +47% higher risk;
- PCORnet (National Patient-Centered Clinical Research Network) dataset: +14% higher risk;
- PEDSnet (child-focused) dataset: 3.14 times higher risk.
COVID-Related Excess Death and Sickness
This paper from Italy (2025-07-01) reports that cancer rates in Calabria (in southern Italy, and has about 10% of Italy’s population) went up significantly post-pandemic vs. pre-pandemic. To be slightly more specific, there was a discontinuity in 2021 — which is when the Alpha and Delta waves hit.
The study reports that
- the cancer rate went up from 14.3 per 1000 person-years in the years 2017–2019 to 23.1 per 1000 person-years in the period 2020–2022;
- women’s cancer rates increased more than men’s;
- brain and skin cancers increased most — by 300% in 2022 compared to 2017;
- cancer rates for people under 65 increased more than for people over 65.
I can construct a story that skin cancer rates went up if people entertained themselves outside instead of inside, but that doesn’t explain why brain cancer rates went up. (Also, from what I understand about Italy, they were not allowed to leave their houses for exercise. My Italian tutor told me that from March 2020 to May 2020 and then again in the winter, only one member of her household was allowed to go up to 1 km away for 1 hour per week to go shopping or walk the dog. If you wanted to go to a medical appointment, you had to file a form.)
This press release (2025-07-02) by an insurance company says that insurance claims for circulatory system claims have risen by 60% “post-COVID”. (I couldn’t tell if they meant “since the start of COVID”, “since the lifting of the state of emergency”, or what.)
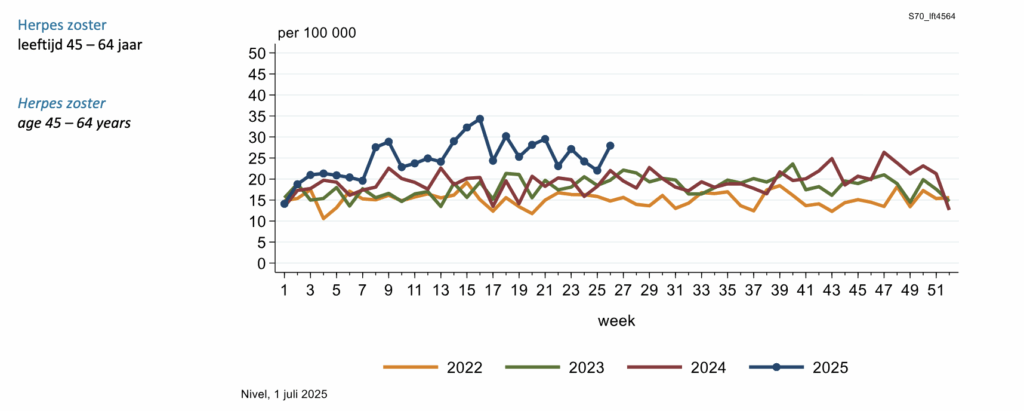
This blog post (2025-06-28) points out an increase in shingles in younger people (under 65) since COVID-19 hit, and wonders if the increase in shingles in non-elderly people is because COVID wrecked our immune systems.
For evidence that shingles is increasing, he pointed to this web page (2025-07-01) from Netherlands Institute for Health Services Research. It’s hard to see in the early weeks of the years (on the left), but if you look later in the years, 2023 (green) is distinctly higher than 2022 (yellow) and 2024 (red) is higher than 2023. If you look at 2025 (blue), it is way higher than the other years.
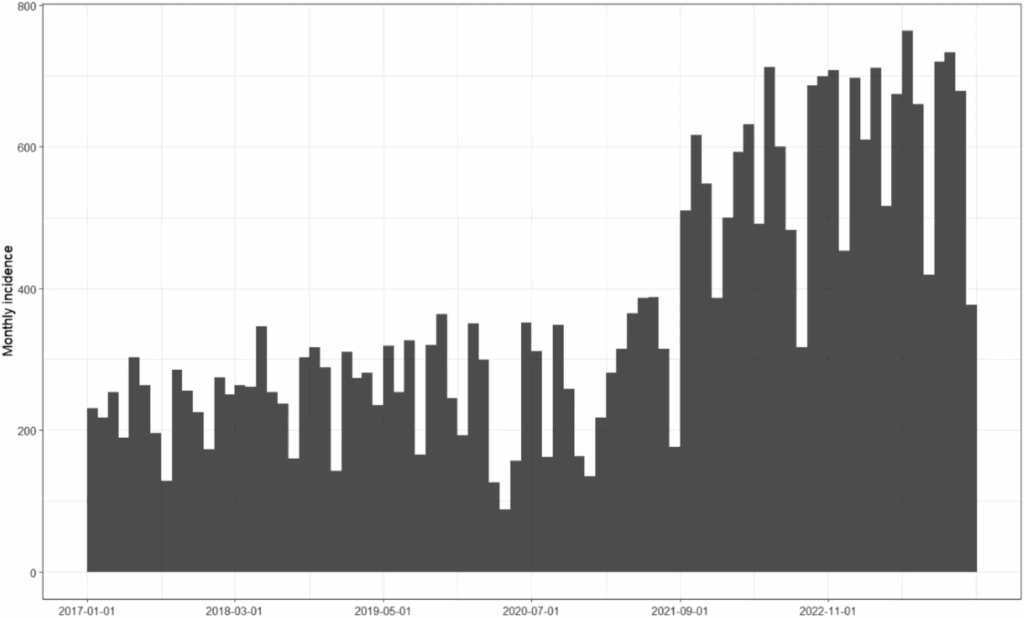
This paper from USA (2025-03-10) reports that the incidence of irritable bowel system rose 63%, from 6.1% in May 2020 to 11.0% in May 2022.
🧠 I am kind of bored with papers that use various imaging mechanisms to look at the details of how COVID-19 and/or Long COVID change the brain. The papers talk about which specific areas of the brain have shrunk, or got bigger, or have higher values of something, and that don’t mean anything to me. I’m not an immunologist, but I am really not a neuroscientist.
Do not think that me not mentioning such papers means they have dried up. DEFINITELY NOT. These papers come up relatively frequently, like this one from Italy (2025-07-02) and this one from China (2025-07-02). I just don’t talk about them.
Transmission
📆🌊 This preprint from USA (2025-06-27) does some mathematical modelling and says that you can model at the state or country level when COVID-19 waves happen using wavelets. They say that there are two components: an annual wavelet and a sub-annual wavelet. The annual one is more pronounced in places with cold weather, and the sub-annual one is more pronounced in places with warm weather. Tropical places (Hawaii, Puerto Rico, and the Virgin Islands) show essentially no annual component, and the areas around the Great Lakes show very little sub-annual component.
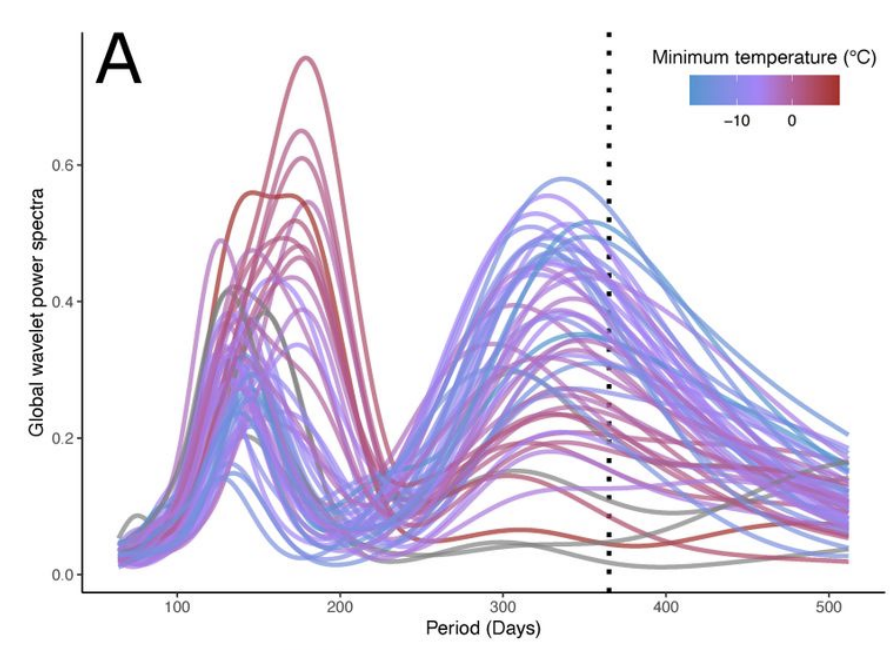
They then did some fiddling around with epidemiology models and were able to model a sub-annual wave if
- there is no long-term immunity,
- immunity wanes relatively sharply, and
- the half-life of immunity is short — although it sounded to me (reading between the lines) like these models were relatively sensitive to initial conditions.
This does look like something interesting is going on here.
But.
I don’t think the model is useful for predicting when waves happen. Here’s the historical chart of cases (red) and number in hospital (black) in BC, with my eyeball estimation of wave peaks marked by blue lines:
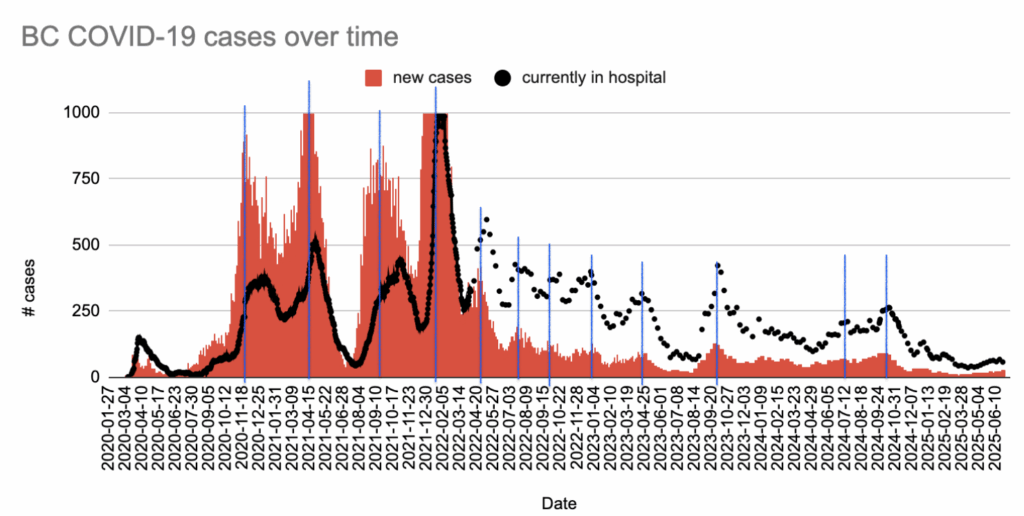
It looks to me like there were peaks at about
- 2020-11-27 (+138 days)
- 2021-04-14 (+148 days)
- 2021-09-09 (+114 days)
- 2022-01-01 (+112 days)
- 2022-04-23 (+89 days)
- 2022-07-21 (+76 days)
- 2022-10-05 (+87 days)
- 2022-12-31 (+117 days)
- 2023-04-27 (+154 days)
- 2023-09-28 (+379 days)
- 2024-10-11 (+80 days)
- 2024-12-30 (maybe? unmarked) (+80 days)
This doesn’t look like there’s any periodicity, even if you say there’s an annual period plus a shorter-term period.
Part of the trouble is defining what a wave is. Is the little bump at 2024-12-30 the peak of a wave? Are all the bumps peaking at about 2022-07-21 and 2022-10-05 waves?
But also, it looks to me like there weren’t any waves between 2023-09-28 and 2024-10-11 — more than 12 months. If there’s an annual wave, um, where did it go?
The paper’s model used data from roughly the first two years of the pandemic. Maybe it was a good model for then, but things have changed somehow (vaccines? different strains? no longer masking?) and so the model no longer applies?
It is clear that — regardless of how many times Dr. Henry uses the word “seasonal” — COVID-19 is not “seasonal”.
🗣️‼️ This older Letter to the Editor (2021-07-15) puts forth an interesting hypothesis: that people get infected in the nose and then later speak, generate aerosols, and breathe their own aerosols into their lungs, making their disease worse. They say:
- Big droplets are too big to get into the lungs (they deposit in the upper respiratory tract instead);
- People expel droplets when they speak;
- After a very short time, the droplets evaporate enough to become aerosols;
- Aerosols can get into the lungs;
- Cloth masks catch the droplets before they become aerosols.
They pointed to research which shows that people who wear cloth masks don’t get as sick, and they also did some research with Deaf people who’d been infected with COVID: the researchers interviewed them about how much they wore masks, how much they vocalized, and how severe their COVID-19 infections were. They found that the more the deaf patients wore masks, the milder their symptoms; the less they vocalized, the milder their symptoms!
So perhaps this means that if you get a COVID-19 infection, you should shut up.
🧑🍳🧑💼 This preprint from UK (2025-06-18) found that the introduction of COVID-19 into care homes was more directly related to the number of non-care workers at the home, and the effect was not small:
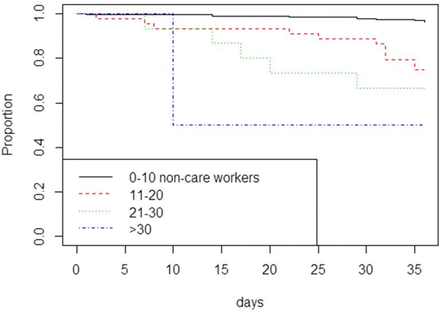
The authors think that maybe it had to do with less access to or use of PPE, or that non-care workers moved between care homes more.
😷 Once COVID-19 got into a care home, how well it spread was affected by how available PPE was.
Pathology
This paper from USA (2025-07-04) reports that, in tissues grown from human retinal tissues, SARS-CoV-2 induces amyloid-β protein aggregates. (Note that human retinas are part of the central nervous system.) Beta amyloid plaques are also seen in Alzheimer’s. 😬
Unforeseen Side Effects
Apparently humans have an ☀️”optimism bias”, where they over-value optimistic data and under-value pessimistic data. ⛈️This paper from France (2025-06-30) reports that “during the pandemic” (which they meant as 2020 and 2021), people had less of an optimism bias than people pre-pandemic and in 2022.
Medical System
🎖️ This article (2025-06-30) reports that both Dr. Bonnie Henry and Dr. Teresa Tam were appointed to Order of Canada. I haven’t decided how I feel about this. I’m kind of mad at Dr. Henry for enabling the “you do you” attitude, but everybody is mad at Dr. Henry. Either she did too much or didn’t do enough, such is the curse of public health.
She did do some things right. While she did close a bunch of indoor/dangerous not-absolutely-essential establishments (nightclubs, indoor dining, hairdressers, churches, nightclubs, banquet halls, gyms, etc.), she left open essential places (grocery stores, pharmacies, etc.) and allowed/encouraged safer options, e.g. restaurant takeout and delivery. She also always always always encouraged us to go outside, both for recreation and for socializing. She asked that people think twice about driving to other cities, but never forbade it.
This was a lot “lighter touch” than some places. (See my discussion of the restrictions in Italy, above, for example. UK also had very strict travel restrictions.)
Recommended Reading
This investigative report by Global News (2025-07-02) says that the Vaccine Injury Support Program is all f’d up — that the company they outsourced it too has spent almost twice the amount on administrative expenses than it has disbursed to people who were harmed by the vaccine.
I love vaccines, but I absolutely, absolutely believe that we should take care of people who were harmed by them. Not only is it The Right Thing To Do, it’s bad for society if people think we’re not going to take care of them if they get a shot. (NB: The article mentions that only 0.011% of people had a serious reaction.)
Influenza
Vaccines
This press release by Moderna (2025-06-30) reports that their flu shot did really well against multiple influenza strains. Its relative vaccine effectiveness (compared to one of the flu shots in common use) was 26%.
Measles
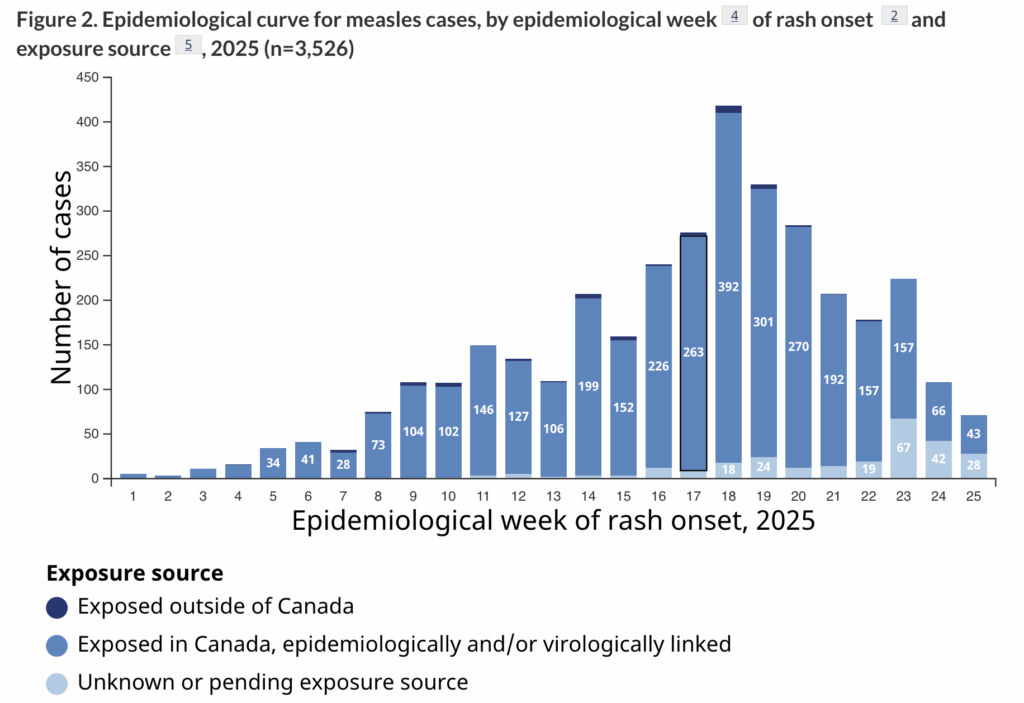
Transmission
This Government of Canada measles and rubella page (2025-06-30) reports that Canada had 145 new measles cases in the week ending 2025-06-21.
- 8 in BC;
- 104 in Alberta;
- 30 in Ontario;
- 3 in Manitoba.
The good news is that the rate of infection is slowing:
H5N1
Transmission
I haven’t posted about bird flu in the USA in a while, and that’s because I haven’t really heard much. I don’t know if the outbreak in the US is dying down or if the Trump administration decided to clamp down on data. 🙁
This article (2025-06-39) reports that Cambodia has been having a lot of human cases, including six in June.
Policy
This article (2025-07-03) reports that RFK Jr is saying they should let H5N1 rip through poultry “to identify the birds that survive, which are the birds that probably have a genetic inclination for immunity”. Many people think this is a really bad idea.