
Omni-Testing
😮🩸‼️🎉 This paper (2025-02-21) reports on a method of sequencing the genomes of T-cells and B-cells from a patient’s blood sample which allows them to diagnose with great accuracy what pathogens the patient has been exposed to. Apparently B cells and T cells don’t have the genome of the rest of the body, but randomly shuffled genes, at least in the part which builds the receptors. That randomization lets the body build a vast library of receptors, some of which will grab on to pieces of pathogens and kill them.
To use this as a diagnostic, they do need to be able to recognize which gene sequences correspond to which diseases, but they have built an AI which can recognize a genome for a specific disease given training data from people with that disease. They now have genetic data which lets them recognize COVID-19, HIV, lupus, type 1 diabetes, and recent flu vaccination with 93% sensitivity and 90% specificity. (In lay terms, that means if the test says you have it, there’s a 93% chance you have it; if the test says you don’t have it, there’s a 90% chance you don’t have it.)
Yes, they will need to do this training for All The Diseases, but IIUC, they’ll only have to do it once per disease, and they did this training with only about 500 people… so looks to me like there’s not huge barriers to just cranking through the top diseases/conditions at a rapid rate. I bet that in five years, I’ll be able to give a blood sample and have them tell me if I have (or had) Zika or malaria or typhus.
This is a big f deal. How many f years have humans wasted getting a proper diagnosis???? How many people have died because of a misdiagnosis?
I also wonder if the tests might end up being even more accurate than advertised. After all, the AI was trained on data from people who were diagnosed by humans; I would not be surprised if a relatively high percentage of the people in the training dataset were misdiagnosed.
Multi-Antiviral Chewing Gum
😮🎉 This article (2025-04-15) about this paper (2024-12-10) reports that a chewing gum made from the Lablab bean neutralizes at least two herpes simplex viruses, two influenza viruses, and (from this older paper from 2022-09-01) a common-cold coronavirus (HCoV-OC43).
Apparently, there’s a protein (FRIL) in the lablab bean which traps viruses. It doesn’t kill them, it just kind of wraps them up. Lablab beans have been used as food for a very long time, so chewing gum made with lablab bean powder is unlikely to be dangerous.
COVID-19
Long COVID
This survey-based paper from China (2025-04-15) found that a COVID-19 reinfection increased the risk of Long COVID by 3.56 times compared to people who were not reinfected.
Interestingly, they said that using traditional Chinese medicine for symptoms reduced the risk of having severe Long COVID (enough to interfere with daily activities) by 49%!
In contrast to many other studies, they said that people over 65 were 63% more likely to get Long COVID than people under 65.
This paper using data from Argentina, Brazil, Canada, Colombia, Ecuador, Egypt, India, Nepal, Pakistan, Philippines, Russia, Saudi Arabia, South Africa and the United Arab Emirates (2025-04-15) reported on Long COVID in places we usually don’t get data from, and the differences surprised me.
They found that ~25% of people who had COVID-19 infections got Long COVID. So far, no surprise. But then they said that men, people from low-income countries, and older people (like the study above!) were more likely to have Long COVID, and that smokers, diabetics, and people with prior lung disease were less likely to get Long COVID!
They also said that different ethnic groups had different prevalence, with Arab/North African people having the highest prevalence at 36%. 😬
👃 This pre-proof paper from Italy (2025-04-17) reports that most people who lose their sense of smell after a COVID-19 infection regain their smell within the first year. 92.3% were recovered at the four-year mark. Being younger and getting smell training were both associated with a better recovery.
🩸 This paper from UK (2025-04-17) reports that people who got Long COVID after an infection had anti-nucleocapsid antibodies at 200 days, while people who had an infection but did not get Long COVID did not. That looks to me like there’s a persistent infection in people with Long COVID.
COVID-Related Excess Deaths and Sickness
👶 This paper from USA (2025-04-11) reports that children who got a COVID-19 infection were 17% more likely to get a diagnosis of chronic kidney disease within the next six months.
🧠 This paper from India (2025-04-13) reports that in a small study of medical students, those that had had mild COVID-19 infections did not score any worse on cognitive tests than those who did not have COVID-19 infections.
Transmission
📱😮 This paper (2025-04-09) looked at the difference in how Android users and iPhone users experienced the pandemic, based on their usage of the CoronaCheck app. Android users were younger, more male, and less educated than iPhone users, and had more then twice the number of suspected COVID-19 infections.
⌚️ This paper from USA (2025-03-04) models the effect of smartwatches diagnosing illness on R, the reproduction number. (Reminder: if R is less than 1, the illness dies out. If it is over than one, it spreads. If it is a lot more than 1, life gets really interesting.) The idea is if N% of people get a smartwatch notification and stay home, then R will drop by X. Here’s what they found R values would be for 66% and 75% reductions in human contacts:
| No reduction | –66% contacts | –75% contacts | |
| COVID Classic | 2.55 | 1.37 | 1.16 |
| Delta | 1.54 | 0.82 | 0.69 |
| Omicron | 4.15 | 2.20 | 1.87 |
| Influenza | 1.28 | 0.74 | 0.64 |
I have some beefs with this paper. It isn’t clear if the “no smartwatch reduction” R values are for what the R is if zero mitigation measures are taken, or what R actually was in practice with significant mitigation measures taken? What point in time is the Omicron R for (because I guarantee you, Omicron’s R-value is not 4.15 right now).
I also don’t believe that a lot of people are going to stay home if a smartwatch tells them to (even if they did wear a watch). I have lost faith in humanity. 🙁
😷 On 2022-09-27, Singapore stopped requiring full PPE for healthcare workers (HCW) when attending to patients with suspected or confirmed COVID-19. Instead of gowns, face shields, gloves, and N95 masks, they only required N95 masks after that. Good news: the change did not make more HCWs sick. Before the switch, HCWs caught COVID-19 2.6 times more frequently than the general population, and after the switch, they caught COVID-19 at only 1.5 times more frequently. (I find it interesting that the infection rate went down after the PPE de-escalation. I wonder if maybe before the switch, HCWs decided to look the other way if someone might have COVID-19 because they just didn’t want to go through all the hassle of donning gown/face shield/gloves.)
They also saved 4 gowns per patient-day🎉 which translated into USD$333,970 per year. That’s a lot of waste.
This paper from South Korea (2025-04-17) reports, surprisingly, that as the number of nurses per patient increases, so does the number of hospital-acquired infections. If I understand this paper correctly, it sure looks to me like nurses are significant spreaders of COVID-19.
Pathology
🧬 This preprint from Singapore (2025-04-15) reports that people who had two copies of variant 252F of the rs2980619 gene had about four times the risk of a severe case of COVID-19.
This paper from China (2025-04-15) reports on several things they found that predict that a case of COVID-19 will be severe. In addition to Western medicine biomarkers, they looked at traditional Chinese medicine biomarkers and found that in addition to age, these biomarkers correlated with severe cases:
- elevated procalcitonin;
- 😮👅 thick tongue fur (that white film on your tongue);
- 😮👅 “fat tongue shape”.
🦠 This pre-proof paper from China (2025-04-17) reports that the gut biome changed markedly in a number of previously healthy individuals after a mild infection of COVID-19.
Treatments
🎉 This paper from China (2025-04-14) reports that among people hospitalized for COVID-19, those who got Meplazumab (a monoclonal antibody usually used for asthma(!)) had a 28-day mortality rate that was about a quarter of that of people who got a placebo.
🎉 This paper from China (2025-04-05) reports that among patients over 60 hospitalized for COVID-19, those who got azvudine (a reverse-transcriptase inhibitor approved against COVID-19 in China) had a 29% lower all-cause mortality than people who got Paxlovid.
💊🩸 This paper from UK (2025-04-05) reports that oral anti-coagulants increase the risk of Long COVID. Note that there are two main classes of oral anti-coagulants: direct-action oral anti-coagulants (DOAC, e.g. Eliquis) and vitamin K antagonists (VKA, e.g. warfarin).
- COVID-positive people who took DOACs had a 50% higher risk of Long COVID than people who did not take an anti-coagulant.
- COVID-positive people who took VKAs had a 98% higher risk of Long COVID than people who did not take an anti-coagulant.
- COVID-positive people who took DOACs had a 31% higher risk of Long COVID than people who took VKAs.
Vaccines
💉🎉 This slide deck from Moderna’s presentation to the CDC’s Advisory Committee on Immunization Practices discusses a study of Spikevax (Moderna Classic) vs. their new mRNA-1283 in adults. Both formulations were bivalent, based COVID Classic and BA.4/BA.5 variants.
It is not entirely clear from the presentation how the two vaccines are different, but it looks like the new one targets the N-terminal domain (NTD) as well as the receptor binding domain (RBD), while the old one only targets the RBD — which changes more from variant to variant than the NTD.
The slide deck also says that mRNA-1283 will have 1/5th the amount of mRNA in it as Spikevax. You would think that would mean that it would have fewer side effects, but it looked to me like the side effects would be about the same for the systemic issues. Yes, there were fewer side effects at the injection site, but similar levels for the things that would keep me home in bed:
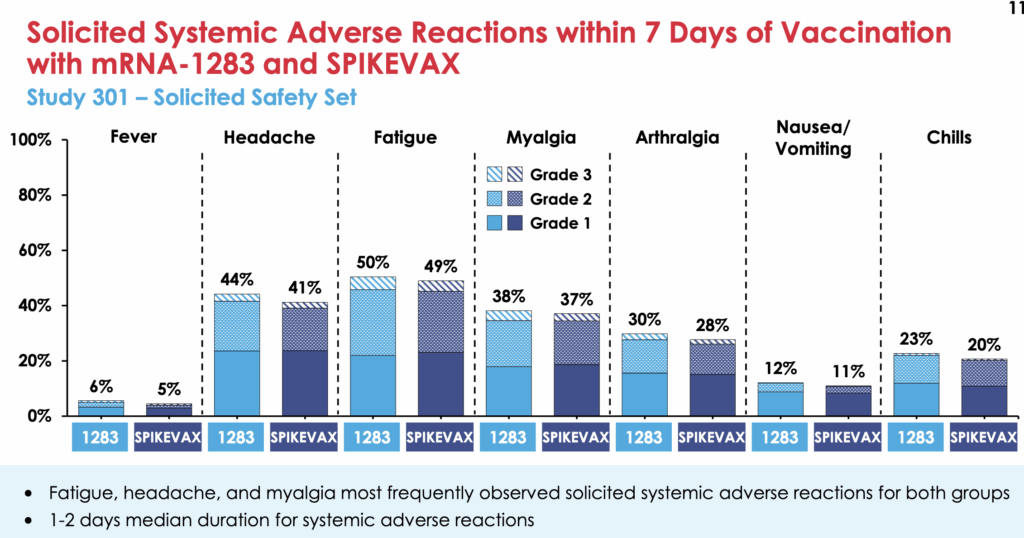
(The rates of get-medical-attention-side-effects was miniscule and the same for both vaccines.)
As far as vaccine effectiveness, the new vax was about a +10% differential better than the old vax. (So in cases where the VE of the old vax is 60%, the new vax is about 70% effective.) The differential was actually more like +13% for people over 65, and — interestingly — minus almost 30% for adolescents! (They do have a caveat that they had a very small sample size for the teens.)
The Wikipedia article on mRNA-1283 says that mRNA-1283 will be fridge-stable and be in pre-filled syringes.
The total cost of vaccination ought to be a lot lower for the new vax, since it has 1/5th the active ingredient and doesn’t need as exotic a cold chain and is in prefilled syringes, but we’ll see if those savings get passed on to the end buyer or not.
I had expected the Advisory Committee on Immunization Practices meeting would also discuss Novavax, but only Moderna was on their agenda (2025-04-15 and 2025-04-16) for COVID-19 vaccines. (I guess Novavax is farther along.)
There was also a presentation on the RSV vaccination’s economic benefits at the ACIP meeting, which included this chart of vaccine effectiveness over time:
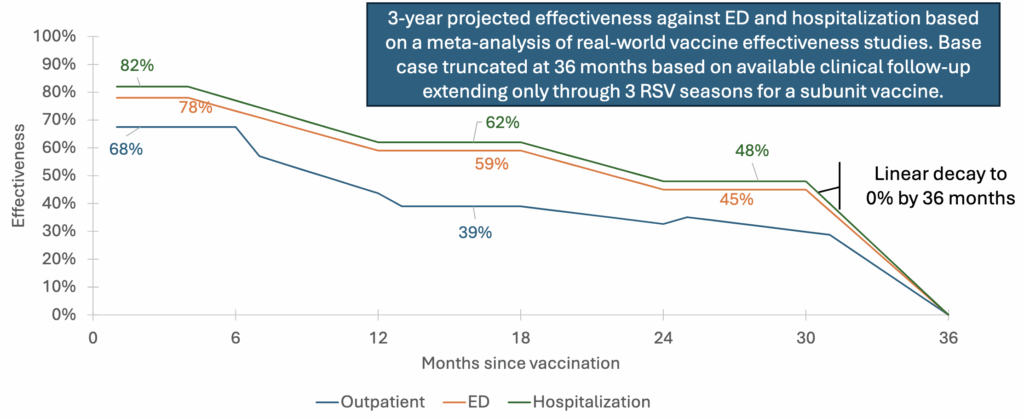
So I guess this means that I’m going to need to get a RSV booster sometime in the next year. This is disappointing but not hugely surprising: the RSV vax was so new that they didn’t know how long it would be good for.
💉🎉 This preprint from South Korea (2025-04-12) reports that Novavax worked better in adolescents than Pfizer. Teens who got Novavax were 41% less likely to seek medical attention for COVID-19 than those who got Pfizer.
💉🎉 This press release by Novavax (2025-04-15) says that a recent study (which looks like it hasn’t been published yet) says that about half as many people who got a dose of Novavax have annoying reactions as people who got a dose of Pfizer.
H5N1
Variants
👶🐦⬛🐦⬛🤧☠️ Last week, I mentioned that a 3 y/o girl in Mexico died of H5N1. This article (2025-04-17) reports that her virus was from the D1.1 genotype — bird bird flu and not cow bird flu. That’s the same genotype that got the Fraser Health teen so sick, and which killed a man in Louisiana.
Transmission
🐦⬛🐄🤧 This article from USA (2025-04-14) reports that there have now been 1009 dairy herds in 17 states infected with H5N1.
Measles
Transmission
There’s quite a bit of measles in Canada, but mostly in Ontario. From the Canada weekly measles and rubella monitoring report (with data through 2025-04-05):
