
Vaccines in General
⭐❗❗ I saw a post on teh socials where the author said that they had talked to people who thought that getting a COVID-19 vaccination too soon after an infection or previous COVID-19 vax was dangerous. Having infections or vaccinations “too close” together is not dangerous. It is less effective, perhaps, but not dangerous. (There’s a guy in Germany who got like 127 COVID-19 shots and was fine.)
This is true of almost all vaccines, not just COVID-19. (Possible exception: dengue — but I am not even sure about that.)
⭐❗❗ You might have heard that whooping cough cases are up hugely in the past few years, both in Canada (22x over prepandemic in Quebec!) and the USA. Whooping cough vaccines (usually) come bundled with tetanus vaccines — the “p” in Tdap is pertussis, the scientific name for whooping cough. If you haven’t gotten a tetanus shot in the past ten years, you should absolutely go get one immediately.
But wait, it gets worse. This (highly knowledgeable) blogger’s post says that whooping cough vaccines are only good for three years. So maybe you want to try to get a Tdap shot even if it’s only been three years. (I have no idea if it is possible to get a Tdap in Canada if it has been less than ten years, however.)
⭐❗❗In the same blog post I referenced immediately above, the author says that mumps immunity is “not what we need it to be” — the mumps strain used is a different strain than what is circulating. However, it looks like a mumps boost will bring protection up to a good level. So getting an additional MMR if you haven’t had any since childhood is a good idea.
⭐❗❗Getting another MMR is also a good idea for measles protection, especially if you were born in the mid-1960s in the USA (and probably Canada also): there was a measles vaccine given from 1963 to 1967 which was not effective.
Note that many universities started requiring another MMR for incoming students in the late 1980s. I was required to get one in 1994 in the US and again in 2005 in Canada.
⭐ The US CDC lowered the age that they recommend that people get a bacterial pneumonia vaccine from 65 to 50. This interview with a doctor says that he’s seeing a lot more pneumonia in middle-aged people than they used to. Me, because I see COVID-19 everywhere, I wonder if maybe COVID-19 has made us more susceptible to pneumonia (and whooping cough).
In BC, the recommended age for a bacterial pneumonia vax is still 65.
⭐❗❗As long as I am talking about it, if you are over 50, go get a shingles vax. Not only do you really not want to get shingles, but the shingles vax appears to cut your risk of Alzheimer’s by about 20% in the six years after the vax.
⭐❗❗Vaccines are one of the most important technological advances ever. They have saved huge numbers of lives. Please stay up-to-date on all of your vaxes!
H5N1
Variants
This article (2024-11-18) reports that the variant of H5N1 which sent a BC teenager to the hospital had mutations which make it more transmissible and more virulent (e.g. deadly). (Reminder: the teen got the bird version of H5N1 (the D1.1 genotype), not the cow version (genotype B3.13).)
The article also reported that all of the teen’s contacts have passed the ten day mark with no signs of onward infection, yay, but that the teen is still in critical care as of 18 November 2024. 😢
According to this paper (2014-06-11) on the Spanish flu, two of the mutations (E627K and E190D) in the BC teen’s H5N1 were also in the Spanish flu. 😬
Note that this paper (2024-10-28) reports there was another case had the E627K and E190D mutations — a Texas dairy worker who was diagnosed in April and only had conjunctivitis. (That strain was pretty transmissible and deadly to ferrets, however.)
So, is it time to panic? Should you be wearing a mask? I think you should already be wearing a mask for COVID, but I don’t think your risk from H5N1 jumped a lot from last week to today. Yes, it is an unpleasant reminder that the H5N1 situation could get really bad for humans — but we knew that already. But it’s not immediate actionable bad news.
I do think you should avoid hanging out in the middle of flocks of birds (or at least wear a mask near them), but that’s been true for several years now.
Transmission
This article (2024-11-18) reports that there have now been 55 human H5N1 infections in the USA.
This article (2024-11-21) reports that a 400 of California’s dairy cattle herds have tested positive for bird flu. This article (2024-11-21) says that 62 Californian herds were confirmed positive just on 21 November 2024, and that so far more than a third of California’s herds have been infected.
Overall, the US has so far found 616 infected herds in 15 states.
This press release from Hawai’i (2024-11-21) reports a poultry flock with H5N1, but genomic analysis (type A3) says that it is a different strain from US cattle and from the BC teen. Its genotype has previously been seen in Alaskan birds, so they expect that it came with migrating birds.
Testing
This article (2024-11-20) reports that Pennsylvania joins Arkansas, Oklahoma, and Massachusetts in mandatory bulk milk tank testing in states with no confirmed dairy cases yet. Go Pennsylvania!
Vaccines
This old paper from Netherlands (2014-07-30) reports that inoculation with a seasonal flu vax (specifically the H1N1 component) might give a little bit of protection against H5N1. The paper says that protection is “transient”, and it’s not clear how much protection it would give, but it makes me think that a seasonal flu vax might keep you from dying, even if it doesn’t keep you from catching the disease.
COVID-19
Long COVID
⭐ This thread (2024-11-16) asserts that Long COVID cost Biden the US presidential election. Briefly, it says that Long COVID took a bunch of people out of the workforce, especially in high-contact professions. That increased the cost of labour, which increased the price of goods. A lot of legal and illegal immigration happened to fill all those empty jobs, which let people get mad about immigration. The combo of inflation and immigration mad a lot of voters mad at the incumbent.
I had not realized just how much immigration there had been in the US in the past four years:

Yes, I know the thread describes the US and not Canada, but last time I checked, Long COVID didn’t care about your nationality. Canada also had a big rise in inflation:

Good news, though, Canada’s inflation (light green) wasn’t as bad as in the US:

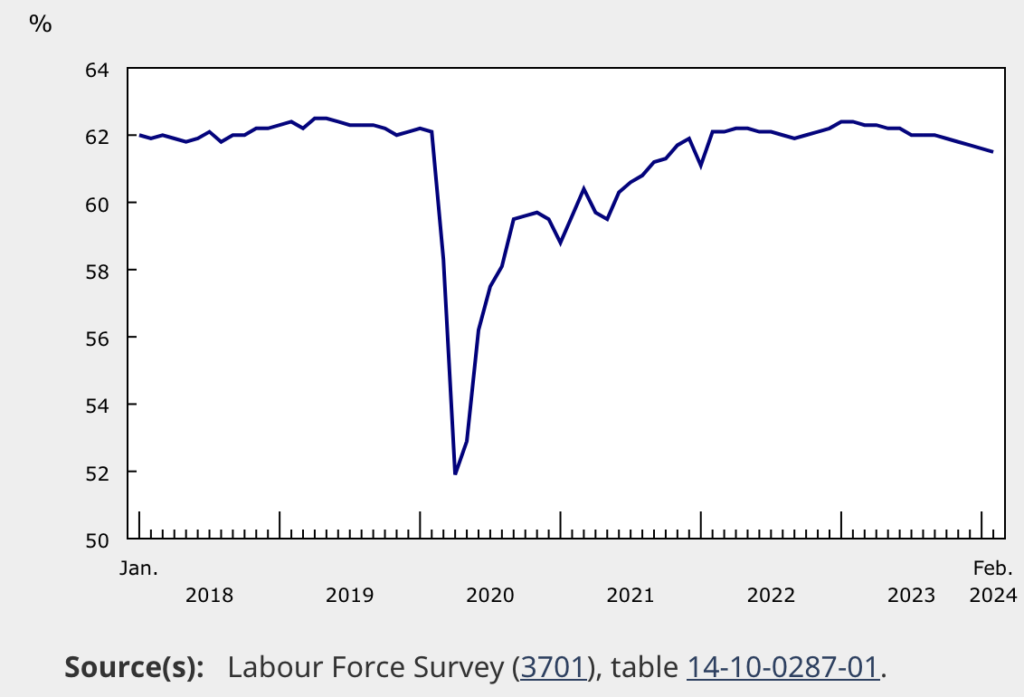
Canada had a big fall in workforce participation percentage during the pandemic; in Jan 2023 it was slightly higher than pre-pandemic, but it has dropped again:
Canada also had a big influx in immigration:

Now, it seems unlikely that this was the only reason for the Democrat’s loss — disinformation probably paid as big a role — but it seems like it was probably a big factor. And, given that the same dynamics have played out in Canada, it might mean that Canadian voters will be mad at the incumbent as well.
Vaccines
⭐ This print from Japan (2024-11-20) looks at how well JN.1-based mRNA vaccines do against JN.1 subvariants and XEC. Now, this is not as much use for USA/Canada because we are using mRNA vaccines based on KP.2 (a child of JN.1), but something that was interesting is that the JN.1 vax seems to be leading us away from imprinting.
When you get a series of vaccinations, the first one you get matters. Your immune system “imprints” on that one, and shows a preference for fighting that one. It’s like if your first martial arts training was with knives, you might be more tempted to use the bayonet on your rifle than to shot it, while people who first got gun training would be more inclined to shoot than stab. It can take more training (corresponding to more vaxes in this metaphor) to get the knife-training instincts beaten out of the knife-trained fighters.
The authors of this study had previously found that people who had gotten an XBB.1.5 booster didn’t have as good a protection against XBB.1.5 as against B.1.1 — a strain which was closer to the original Covid Classic. This time, however, they found that people who got the JN.1 booster did better against XBB.1.5 than against B.1.1, so it looks like the tide has shifted. 🎉
Testing
For both of my readers who live in the USA, a reminder that if you haven’t gotten your four free rapid tests via the mail, you probably should do that before January 20th. There’s no telling how long the program will last after Trump gets sworn in.
For those of you who live in BC, free rapid tests are still available at pharmacies. I grabbed two boxes a few days ago.
Transmission
This paper from USA (2024-11-11) reports that after Omicron appeared, 21% of reinfections happened within six months of the first infection. In other words, an infection doesn’t always protect you for even six months.
This paper from Brazil reports that 19.1% of tested mammals at a zoo were positive for COVID after visitors were readmitted. A lower number — but still non-zero — of them tested positive even during the period when there were no visitors, suggesting that the zookeepers gave it to the animals; they think that the higher post-visitor COVID-19 levels are due to visitors making the zookeepers sick more often.
Treatments
🎉 This paper from China (2024-11-07) reports that simnotrelvir plus ritonavir (S/R) worked very well as an anti-viral treatment. The control group was at about ten times higher risk of hospitalization than the S/R group! (Simnotrelvir is a protease inhibitor; ritonavir is (if I understand correctly) a drug which boosts the activity of the other drug. Ritonavir is used in HIV therapies and as one of the ingredients in Paxlovid.)
⭐ This press release (2024-11-13) says that BC 007 did no better than placebo in a Phase 2 trial. This makes me sad because it initially looked like a magic bullet: four people with Long COVID had full recoveries with BC 007 back in 2021. I had been watching and hoping, but alas, it was not magic. 🙁
⭐ This paper from Czechia (2024-11-20) reports that molnupiravir is hugely useful for high-risk adults with mild COVID-19 symptoms. They found that in high-risk patients who were given molnupiravir quickly, the 30-day risk of COVID-related death dropped in half and the 30-day all-cause mortality risk dropped by 42% compared to matched controls who didn’t get the drug. (Patients were considered high-risk if they were older than 65 or obese or had underlying illnesses.) The effectiveness was the same for vaccinated and unvaccinated patients.
Patients who were under 65 or who started molnupiravir more than 4 days after diagnosis did not see any benefit.
This preprint from China (2024-11-10) found that pemivibart — a monoclonal antibody approved in the US but not Canada — works great against JN.1 but kinda sucks against KP.3.1.1 and XEC. 🙁
Pathology
⭐🎉 This is wild. This paper (2024-11-15) reports that some cancer patients with COVID-19 have their tumours shrink, and they figured out why! Apparently, cancer hijacks a part of the immune system called monocytes to protect the tumour, but inflammation — like COVID-19 causes — de-hijacks the monocytes, so that the immune system can go back to attacking the tumour! Furthermore, it looks like the cascade of things de-hijacking the monocytes is something that can be mimicked with drugs. So the pandemic might actually have a silver lining of improving cancer treatments!
Floss your teeth! This older article from Qatar (2021-02-01) reports that people with periodontitis had much higher risks of severe outcomes from COVID-19 than people without periodontitis:
- Almost NINE TIMES the risk of death;
- 3.54 times the risk of hospitalization;
- 4.57 times the risk of going on a ventilator.
Tip: tie your floss in a loop before flossing. That makes it much easier to keep tension on the line without cutting off circulation in your pinkies.
⭐ This paper from California (2024-11-07) reports that people who lived within a kilometre to oil and gas wells were more susceptible to COVID-19, compared to demographically similar communities farther away. People who were in communities in the top third of oil and gas production had 34% higher case rates and 55% higher mortality rates than communities with no production.
Air quality matters, folks!
Mitigation Measures
⭐ I have heard anecdotes about people disliking other people wearing masks, which I found strange. Well, this paper (2024-11-11) reports that people are less accurate at recognizing emotions (especially sadness) in masked people, and that it takes more brain effort to recognize emotions.
Research
This site is a search engine for COVID-19 research preprints.
Recommended Reading
This article and this Bsky thread talk about mouthwash as a COVID-prevention technique.
Mpox
Transmission
This press release (2024-11-16) reports that they have identified a Clade 1 case in California — someone who visited Eastern Africa and came home with a souvenir. (Clade 1 is the scarier clade, clade 2 is the less scary one.)
Vaccines
🎉 This press release (2024-11-19) from the World Health Organization authorizes a second mpox vaccine, the Japanese attenuated vaccinia vaccine LC16m8. This is the first vax approved for use in children (as young as 1 year old), and the government of Japan is donating a little over 3 million doses. 🎉