
This article reports that the World Health Organization has declared mpox to be a pandemic, so I guess I will occasionally cover mpox as well. Honestly, world, can we stop having so many pandemics?!?!
This article (2024-08-13) reports that World Health Organisation has added Black Death, H5N1 and mpox to its priority pathogens list. That sounds like an administrative yawner, but it’s actually important: when a disease gets on its list, that makes it a lot easier to get funding: researchers can say, “And this is on WHO’s priority pathogens list!”
WHO only started making this list in 2017, but already it has a big win. In 2017, they put MERS on the list, and some companies started researching a vaccine, including AZ and Moderna. The COVID-19 vaccines were direct pivots from research on MERS that was probably made possible in part because it was on the priority list.
Moral of the story: sometimes administrative yawners save millions of lives.
COVID-19
Mitigation Measures
Last week I said that Nassau County, NY had banned masks. Apparently the law was passed but not signed. (No, I don’t know the difference at the county level.) This article says that this week they signed the law, putting it into effect.
This paper from USA (2024-07-30) reports that, basically, people who take mitigation measures are nicer people than those who do not.
- People who always masked were significantly higher in compassion for others and significantly lower in sadism compared to those who did not always wear masks.
- People who always socially distanced were significantly higher in openness, compassion for others, and conscientiousness compared to those who did not.
- People who hoarded resources (e.g. cleaning products, hand sanitizer, personal protection equipment, food items, toilet paper) were significantly lower in agreeableness than those who did not hoard.
This paper from USA (2024-08-14) found that about ~3.5% of healthcare workers got vaccinated as a direct result of vaccine mandates.
This paper from Italy (2024-08-12) reports that the people who were seen at a hospital in Bergamo, Italy, for COVID-19 in in the very first wave (before September 2020) had not well recovered later (median time between discharge and evaluation was 81 days):
- 31% had possible PTSD. (Which honestly? Seems totally understandable to me. Bergamo was very badly hit. VERY. The hospital was completely overrun, with patients in the hallways, nobody knew anything, and a lot of people died. I think a lot of people in Italy who didn’t even get COVID-19 probably have PTSD from how bad it was.)
- 41.9% had lingering symptoms.
- 19.6% had reduced lung capacity.
- People of low socio-economic status (SES) were 45% more likely to have mobility limitations and 53% more likely to have physical pain than those of higher SES.
I and many COVID-cautious people have been puzzled at why other people aren’t (in our opinion) adequately concerned about COVID-19. Then I learned about Normalcy Bias — a cognitive bias which leads people to disbelieve or minimize threat warnings, and omg that’s why!
Long COVID
You might see me posting more information about ME/CFS research. ME/CFS might be different from (extreme) Long COVID, but it might not be; I think the jury is out on that. Furthermore, I have started to see quite a few papers which will give ME/CFS diagnoses to people with Long COVID. This is reasonable, given that many (most? all?) ME/CFS happens after a viral infection, so they are just lumping post-COVID ME/CFS in with all the other post-viral ME/CFSes. Thus, I am going to lump ME/CFS in with Long COVID until/unless the scientific community decides they are actually different things.
This paper from USA found that 30% of post-menopausal women who had had COVID-19 infections got Long COVID.
There were several papers which found measurable differences between people with Long COVID or ME/CFS and healthy controls. They don’t always know what the differences mean, but having measurable differences means that 1) it’s useful ammunition to use against people who think that Long COVID and/or ME/CFS patients are making it up and 2) useful for clinical assessments.
- This paper from Spain (2024-08-02) reports that people with Long COVID have slower eye motions and more fixations in reading tasks. (This looks like a really cheap, easy, and non-invasive diagnostic test!)
- This paper from Australia (2024-08-07) reports that MRIs can see a difference between ME/CFS patients and healthy (but sedentary) controls. Subjects did a groups of tasks, rested for a little bit, and then did the tasks again. Healthy controls’ brain activity was lower the second time through, while the ME/CFS cohort had higher activity levels.
- This paper from Netherlands (2024-08-04) reports that ME/CFS patient have reduced blood flow to the brain during tilt tests. This suggests that there is something messed up with vasodilation/constriction regulation. People had worse ME/CFS had worse bloodflow.
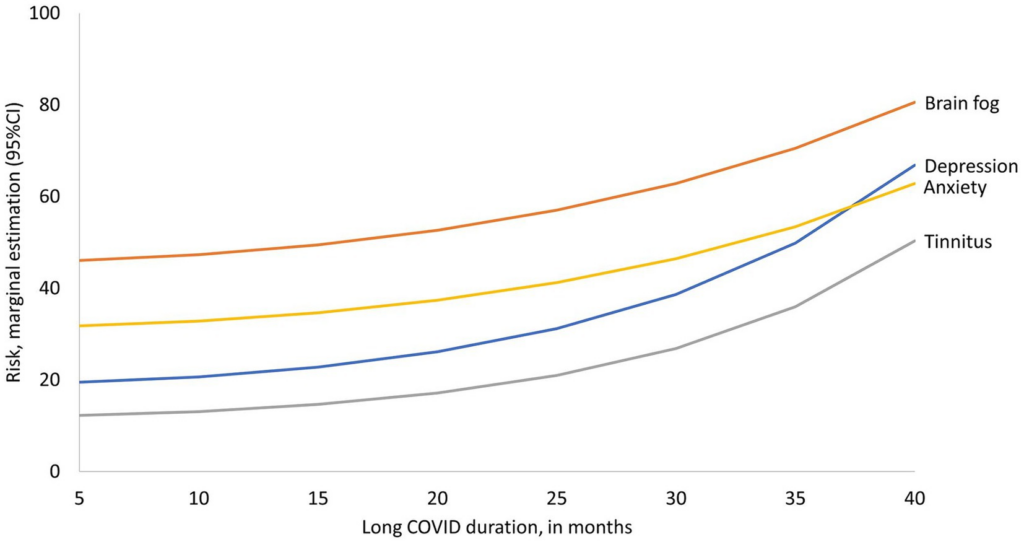
This paper from USA and Columbia (2024-08-15) reports that Long COVID has long-lasting impacts, even after three years.
This paper from USA (2024-07-29) reports that at three months, 40% of people who had had COVID-19 infections in the first two years of the pandemic said that they still had at least one symptom. 7.2% said they had missed at least than ten days of work, and 13.9% said they had not returned to work. (I don’t know how the “haven’t returned” number can be higher than the “≥10 days” number. Maybe the ≥10 days people were only ones who did return to work?)
Pathology
I have seen a fair amount of chatter in COVID-cautious circles about how COVID-19 causes lymphopenia — abnormally low level of white blood cells in the blood — and that this will lead to a lot of future cases of Acquired Immune Deficiency Syndrome (AIDS), just like HIV can lead to AIDS. They people expressing this foresee millions of people coming down with AIDS in the future.
I haven’t figured out how much of an issue I believe this is going to be. Certainly, there are not lots of people getting Kaposi’s sarcoma or pneumocystis pneumonia right now. The concern is that it takes a five to ten years for full-blown AIDS to develop, and we just haven’t had COVID-19 for that long. (Yet. We’re getting close to the five year mark.)
There are papers about immune system dysregulation, but a lot of them talk about what happens in severe acute cases (i.e. when people are hospitalized) (like this paper from Indonesia (2020-05-24)). Some papers talk about over-activation of T-cells (like this paper from Switzerland (2022-06-02)) after the acute phase, especially in Long COVID (like this paper from USA (2024-01-11).
We also did not see AIDS develop in people who got SARS1. Their lives sucked and never got back to normal, but I haven’t heard that they got AIDS.
Bottom line: I’m still wait-and-see on this. I am willing to believe that people are getting more colds than they used to (even acknowledging that a lot of “colds” are actually COVID-19). This paper from USA (2023-10-13) reported that kids who had COVID-19 were 40% more likely to get RSV, for example. But I’m not (yet) convinced that COVID-19 infections are going to lead to AIDS.
This paper from Italy (2024-07-24) reports that COVID-19 ages people. The study looked at healthcare workers infected during the first pandemic wave who had mild or asymptomatic COVID-19 cases, and compared them to chronic obstructive pulmonary disease (COPD) patients on a whole bunch of measures of biological age, and found that the COVID-19 patients were biologically “older” than the COPD patients.
Yay! This paper from USA (2024-08-12) reports that US CDC only saw 117 MIS-C cases in 2023, down from a high of more than 200 per week in January 2021.
Vaccines
This article (2024-08-16) reports that Pfizer/BNT’s combo influenza+COVID-19 vaccine Phase 3 trial failed. 🙁 The COVID-19 and influenza A parts worked fine, but the vax didn’t do a good job against influenza B. I’d say “time to go back to the drawing board”, but they already have Rev 2 designed and done with a Phase 2 trial, and Rev 2 apparently is better than their Rev 1 version. They said that Rev 2’s influenza B was good enough, and that its influenza A was even better than before.
This article from USA (2024-08-24) says that the US FDA is expected to sign off on the fall COVID-19 boosters as early as this week. I have no information on when Canada is going to approve, but if you really need a vax, maybe you could run down to the US.
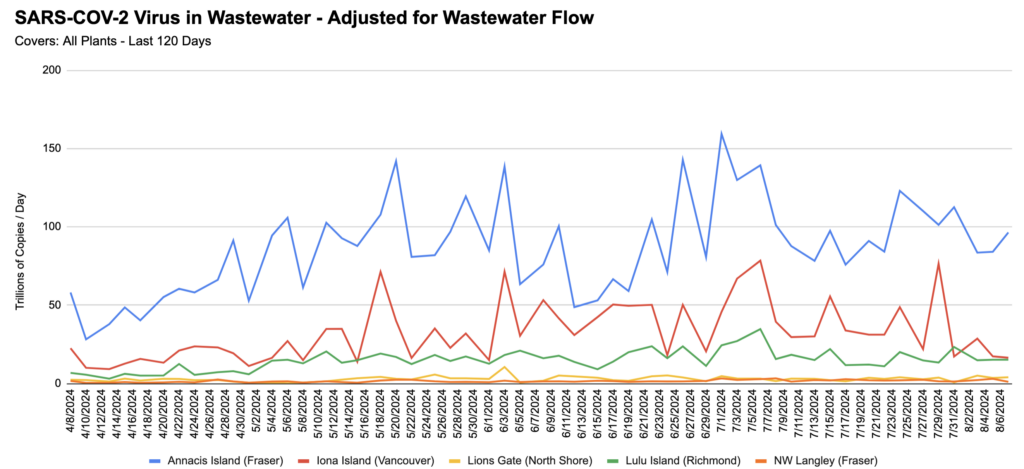
BC Wastewater
From Jeff’s wastewater spreadsheet:
Mpox
Transmission
Mpox is back in the news. This article reports that the World Health Organization has declared mpox in Africa a global emergency. (The vast majority of cases are in Congo and western Africa.)
But wait, it gets worse. The above article reports that 70% of the mpox patients in Congo are in children under 15. Apparently we have known that mpox can spread via aerosols for a while (see this 2022 article; I also found a bunch of other papers which show it spreads by air) but that was underplayed. (The BC CDC mpox page doesn’t mention airborne transmission, for example.)
But wait, it gets worse. This paper from 2013 found that mpox could live in the air for 90 hours.
But wait, it gets worse. This article reports that the version of mpox that got loose the last time you heard about it was clade 2b, the less deadly variant, with a fatality rate of “only” 1% (similar to COVID-19 in the pre-vaccine era). The mpox outbreak this time is a descendant of clade 1, and this variant is more deadly, killing about 10% of people who get it. (NB: Other things I have seen say that the fatality rate is more like 4%, 2% if you get good medical care; see below.)
This article (2023-08-16) reports that they found trace amounts of mpox in NL wastewater. NL is not the only place outside Africa where cases have popped up:
- This article (2024-08-16) reports that Sweden has found a Clade 1 case.
- This article (2024-08-16) reports that mpox has been seen in San Francisco wastewater. (The article didn’t say which clade.)
- This article (2024-08-16) reports that Australia is seeing a spike in mpox cases: only one in 2024 through May, but then 93 since June 1.
- This article (2024-08-16) reports that Pakistan has a case, but they don’t know yet which clade.
Vaccines
This article (2024-08-15) reports that Gavi, the vaccine NGO for low-income countries, has up to $500M it could use to buy mpox vaccines. (Apparently this money is leftover from COVID-19 because of, well, fuckups in getting vaccine out to low-income countries, though the article doesn’t quite phrase it that way.) They do need approval from the World Health Organization, and a request from Congo to ship them shots, and actual shots from the manufacturers (Bavarian Nordic and/or KM Biologics).
The vaccines they are using for mpox are actually smallpox vaccines. (Which is actually the cowpox vaccine, except this fascinating article says the “cowpox” virus in the smallpox vaccine probably actually came from horsepox! The poxes apparently are a lot alike and you can use one of the poxes to vaccinate against a lot of them.)
Per this page, Canada stopped vaccinating in 1972, and Wikipedia says smallpox was declared eradicated in 1980. Thus if you are over 55, you almost certainly got a smallpox vaccination when you were little; if you are under 45, you almost certainly did not. Between 45 and 55, whether you got a vaccination depends on where you were when you were of vaccination age.
So how good is was the smallpox vaccination against mpox? This review paper says that in the early-to-mid-1980s, it was about 85% effective. However, it’s probably less effective now because we are all 40 years older. :-/
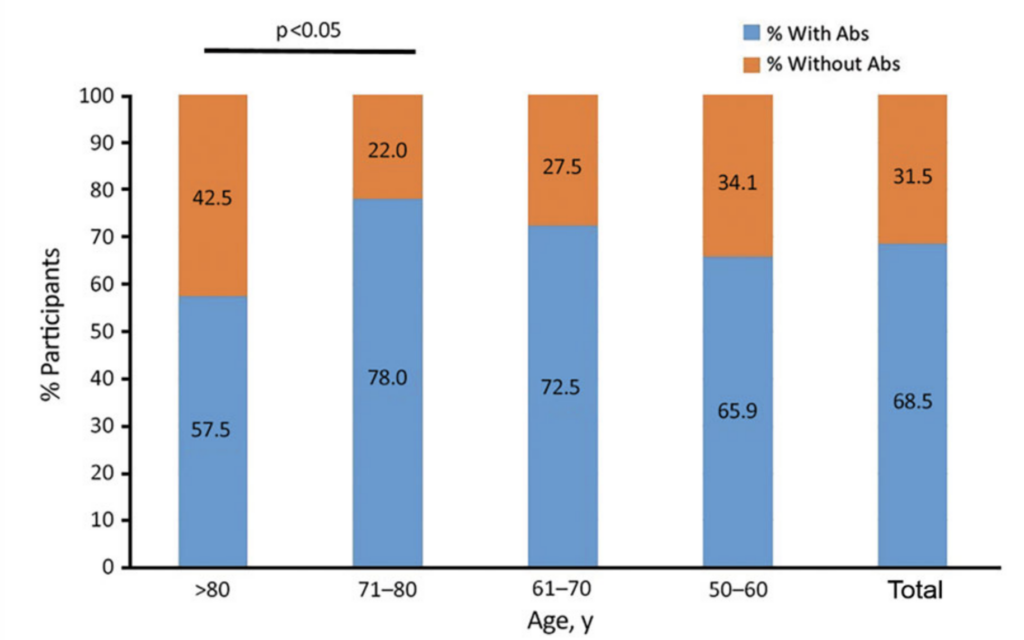
Does it wane? This recent paper from Spain (2023-02-23) reports that 68% of people over 50 had antibodies to smallpox (NB: not mpox!) (well, vaccina, which might be horsepox, see above). 78% of the people over 70 had “smallpox” antibodies.
Other research says that the protection after many years is probably pretty good:
- This paper from USA (2003-08-17), but they also found that anti-smallpox T-cell levels had a half-life of 8-15 years.
- This paper from USA (2003-11-15) says that B cells drop to about the tenth their original level, but after that levels stay stable for more than 50 years.
- This paper from China (2023-09-15) reports that their smallpox-vaccinated population has poor antibody levels, but good non-antibody levels.
- This paper from USA (2008-12) reported that people’s immunity levels basically didn’t drop with age, even up to 88 years. They had some people whose blood had been taken much earlier and stored, so were looking at waning in specific individuals.
While the BC CDC mpox vaccination page carefully says that anybody can get mpox, their eligibility rules say that only men (or people who used to be men) who have sex with multiple people who have sex with multiple people are allowed to get an mpox vaccine. IT’S AIRBORNE, FOLKS!!
This paper (2023-06-14) reports that the immunity from smallpox-vaccinated or mpox infection needs complement (the innate immune system, with things like interferons) to work. COVID-19 damages many things, including the immune system. I have seen chatter about COVID-19 damaging the immune system, and that depressed complement from COVID-19 would thus lead to degraded immunity to mpox. The research that I’ve seen, however, is mostly about the complement system being over-activated, like in this paper (2024-01-24). (That might just be because runaway complement system appears to be a factor in severe COVID-19, and so there are a lot of papers on that which hide papers on under-activation of the complement system from my searching.
This press release (2024-08-16) from Bavarian Nordic says that they have asked the European Union regulators for approval for using their mpox (uh, smallpox) vaccine in adolescents (12-17 y/o).
Speaking of Bavarian Nordic, this article (2024-08-17) reports that the company says they are ramping up their production capability, so they can make 10M doses in 2025. That’s not much compared to, y’know, 8 billion people, but it’s five times what they are going to be able to deliver in 2024.
Treatments
This press release from US NIH (2024-08-15) reports that a clinical trial of tecovirimat failed to show any utility against Clade 1 mpox in Democratic Republic of Congo. Tecovirimat is effective against smallpox, so they were hoping it would work against mpox, but sadly, no such luck.
The good news is that all the study participants (yes, control arm and treatment arm) were required to stay in hospital during the treatment, and the mortality rate was 1.7%, compared to 3.6% or higher in the general DRC population. That shows that good supportive care can cut the mortality rate in half!
This also makes suspect what I said above about Clade 1 having a mortality rate of ~10%.
H5N1
Transmission
This preprint from USA (2024-08-11) found H5N1 viral RNA in 17.4% of samples of retail cheese and butter from 27 states. However, they found zero culturable virus.
Uh-oh. This article from Colorado reports that six housecats have tested positive for H5N1. Owners of two of the cats reported that the cats were indoors-only cats, so the cats probably didn’t catch it from working at the dairy farm. (There is some speculation that the indoor cats might have caught infected mice that got indoors, but they can’t really ask the cats.) Three of the cats were known indoor/outdoor cats. They didn’t say if the sixth cat went outdoors or not.
Testing
This article from USA (2024-08-18) reports that the US FDA is going to start tracking bird flu infection in dairy cows sent to slaughter. (The article says that about 10% of US beef is from dairy cows after they run out of milk; dairy cows usually turn into hamburger.)
Vaccines
This article from USA (2024-08-12) reports that the US Government paid CSL Seqirus to make 4.8M doses of an H5N1 vaccine. The vaccines are done and bottled, but nobody actually knows if they will work or not. CSL Seqirus normally makes people-flu vaccines, and they are just betting that they can use the same process for H5N1. (It has been tested in ferrets, and they have started a human trial.)