
British Columbia is not going to release provincial COVID-19 data next week, so I’m not going to publish a BC post next week. I haven’t decided if I’m going to publish a General post next week or not.
This week, I felt like I didn’t have much material to work with. Partly, it might be that the interesting news got swamped by all the articles saying, “Uh-oh, COVID levels are really high in <location>, maybe if you have a sore throat and stuffy nose, you should consider thinking about at least considering wearing a mask when visit your 97-year-old immunocompromised grandmother”. Meanwhile, social media is full of “Oh blast, I managed to avoid covid for almost four years but my luck finally ran out when I spent twelve hours with my anti-vax inlaws who were sneezing the whole time. What rotten luck! (Okay, I am exaggerating slightly, but not much.)
Long COVID
In this study from USA (2023-12-15) they stuck a sensor into long haulers’ bloodstreams while the patients exercised. They found that the Long COVID patients were getting enough oxygen into the blood, but it wasn’t getting taken out (i.e. used ny cells) fast enough. I am still not a doctor, but from what I can tell, it looks like the mitochondria are f’d or the circulatory system is not getting the blood to the mitochondria properly. (The study showed that the heart wasn’t the problem: it would be vasodilation in the capillaries keeping the blood from getting to the cells.)
This paper from USA (2023-11-27) found that vaccination cut the risk of Long COVID by about half in children who had COVID infections. (This does not count the decreased risk of infection.)
(This was not entirely a given. Children’s immune systems act in some very different ways than adults’ immune systems.)
This paper from Brazil (2023-12-20) found that the heart rate variability decreased in Long COVID patients. That suggests that Long COVID’s autonomic nervous system isn’t working as well. (This could maybe be used as a really cheap way to diagnose Long COVID!)
Pathology
This paper from England (2023-12-14) looked at the case fatality rate (CFR) — i.e. the percentage of people who got sick who then died — between May 2020 and February 2022 as a function of time, age, and vaccination status.
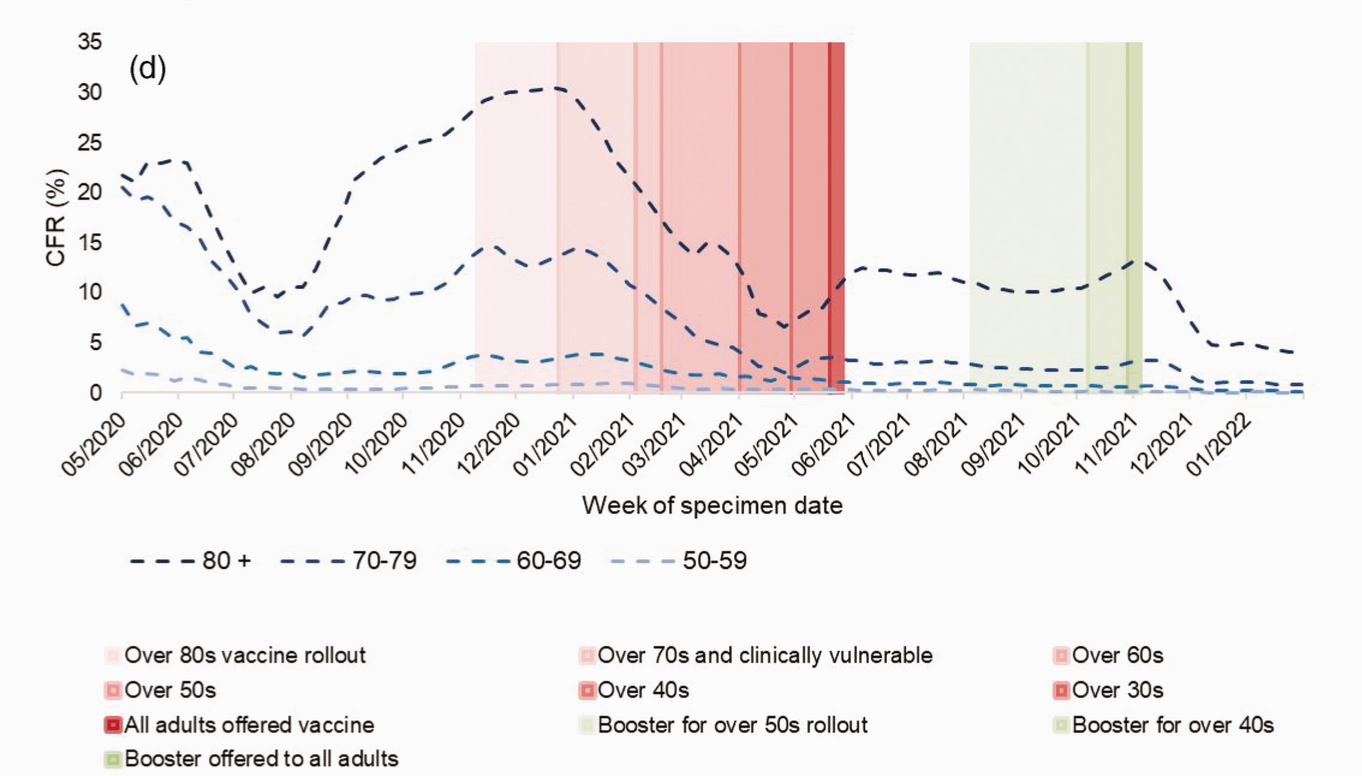
As the chart above shows, before vaccination, the CFR for people over 80 got as high as THIRTY PERCENT. Basically a third of people over 80 who got COVID-19 DIED from it in the winter of 2020.
(Reminder: COVID-19 is not just like the flu!!!)
Overall, the CFR for unvaccinated people with COVID-19 over the entire 20-month time period of the above was 1.65%. Here’s a table to put that in context of influenza both pandemic and normal every-day (“seasonal”) influenza:
| Disease | CFR |
| COVID-19 for unvaccinated | 1.65% |
| COVID-19 for unvaccinated over 80 | 30% |
| Spanish Flu (see also this paper) | 2-3% |
| Influenza pandemic of 1957 | 0.13% |
| Influenza pandemic of 1968 | 0.1% |
| Influenza pandemic of 2008 | 0.05% |
| Non-pandemic (“seasonal”) influenza | 0.16% |
Back to the recent paper from England, they found that the CFR for all vaccinated people over the entire study period was 0.23% (still higher than for the seasonal flu!), but it rose to 0.50% (10x the H1N1 pandemic of 2008) for people who had not gotten a shot in six months.
Broken down by age, the CFRs they found for everybody (i.e. vaxxed and unvaxxed both) over the entire study period, you can see that COVID-19 is really bad for the elderly:
| Age range | COVID-19 CFR |
| 18–29 | 0.01% |
| 30–39 | 0.03% |
| 40–49 | 0.08% |
| 50–59 | 0.27% |
| 60–69 | 1.16% |
| 70–79 | 4.72% |
| 80+ | 16.34% |
Transmission
This paper from Belgium (2023-12-14) found through careful contact tracing of university students, that at the beginning of the Omicron wave, the incubation period looked like this (grey bars for actual data, lines for various fits):

You can see that the incubation period can be very fast!
This paper from UK (2022-11-12) found that sneezing into your elbow reduced the spread of your germs a little bit (especially if there was a sleeve there) but not much.

This paper from UK (2023-12-20) found that the probability of infection grew at ~1.1% per hour in the presence of an infected person.

I would caution you, however, from thinking that that means that brief encounters are always safe. They are not. For example, there were:
- A case in Australia where someone got infected with Delta merely walking past an infected person at a mall.
- A case in a New Zealand quarantine hotel happened when two doors across the hall from each other opened simultaneously for a few seconds.
- A case in a Hong Kong quarantine hotel where transmission happened across a corridor. (They didn’t have a camera like the above NZ case, so don’t know exactly when doors were open.)
Vaccines
There has been a lot of excitement and activity around mucosal vaccines basically ever since we found out that the intramuscular shots don’t last. A few intranasal vaccines have made it through Phase 3 trials, and they, alas, have been underwhelming.
Well, maybe we (humans) have been doing it wrong: it looks like we should be inhaling vax instead of coating our noses with it. Here’s a lay article, which reports:
- This paper from China (2023-12-13) found that a nanoparticle inhaled aerosol vax worked really well in rodents and monkeys.
- This paper from USA (2023-11-08) found that monkeys which were given a booster of a adenovirus-vectored vax (similar to AZ) given by intranasal mist or inhaled aerosol did much better after five months than those who got an intramuscular Moderna bivalent/BA.5.
- This paper from USA (2023-12-14) found that inhaled vax worked a lot better than either intramuscular or liquid intranasal vax in monkeys.
(Aside: One unfortunate thing that the lay article mentions is that mRNA vaccines don’t work very well when inhaled. MRNA vaccines certainly have their drawbacks (particularly the need for ultralow temperatures) but the manufacturers can make them much much faster than traditional methods, which means we can tailor them to new strains much better.)
Back to transmission. Viral load, time, and your susceptibility all matter. The way I think of transmission is that there is someone shooting BB guns (COVID-19) at your front door (your immune system) trying to breach the door.
If you haven’t been vaccinated, it’s like you have a hollow core interior door. If you’ve been vaccinated, it’s like you have a solid-core exterior door. If you are vulnerable, e.g. diabetic/elderly/immunocompromised you’re back to hollow-core if vaccinated, or a shoji screen if not.
The sick person’s viral load is sort of like what kind of gun they have. High viral load is like a fully-automatic BB gun with infinite ammo. Low viral load is like a non-automatic BB gun (still with infinite ammo). Uninfected is like having no ammo.
If you give someone long enough, even if they only have a non-automatic BB gun, they will be able to wear through a solid-core exterior door. If you have a hollow-core interior door and someone has a fully-automatic BB gun, your door is going to get breached pretty fast.
This paper from Italy followed people for two years who had been hospitalized with COVID-19 early in the pandemic and found that vaccination gave more protection than just having been infected: 13.1% of those who had been vaccinated twice got reinfected, 25% of those who had been vaccinated once got reinfected, and 57.1% of the people who not been vaccinated got reinfected.
Now, this might have only been a recency effect. Most of the reinfections happened during the Omicron wave, which hit hardest in Jan 2022 — over 18 months since this cohort had originally gotten infected. I would expect that a recent vaccination would be stronger than an old infection.
The paper also looked at IgM and IgG nucleotide (i.e. from infection, not from vax) antibody waning (“seroreversion”). They found that the IgM nucleotide antibodies were gone in almost all the patients after one year, and about 60% the IgG nucleotide antibodies were gone after two years. (Note: IgG and IgM are mostly found in the blood, while IgA is found in both blood and mucous.)
The paper found that there wasn’t much difference in reinfection rates between people who still had IgG and/or IgM antibodies and those who did not. I interpret that as meaning that IgA is more important in staving off infections.
Variants
With this announcement, the World Health Organization declared JN.1 a Variant of Interest, separate from BA.2.86.
Treatments
This paper from Italy (2022-09-28) found that hospitalized patients who got the regular treatment were 3.4 times more likely to die than patients who took a probiotic containing the K12 strain of Streptococcus salivarius.
This seems awesome BUT I can’t find a source for this probiotic in Canada and most of the Streptococcus salivarius K12 research seems to be done by the same two people.
This paper from Hong Kong (2023-12-16) found that, between 16 March 2022 and 15 January 2023, people who started Paxlovid on the same day or next day as they had symptoms died 23% less often than people who got it 2 or more days later. Within two days was better than within three days; within three days was better than four. Basically, get Paxlovid as fast as you can! (If you qualify, that is.)

This literature review from USA (2023-12-22) found that there wasn’t a big difference in rebound between people who were and were not taking Paxlovid. This double-blind study from USA (2023-12-22) found that Paxlovid patients had a rebound rate of 6.4%–8.4%, while placebo patients had a rate of 5.9%–6.5%. (The figures are ranges because of confidence intervals.)
Testing
This article strongly implies that BTNX — the manufacturers of the “green box” rapid tests — faked the data which the government used to approve the tests. The article strongly implies that those RATs give even more false negatives than other RATs. From the article:

Recommended Reading
This article discusses nasal sprays designed for/marketed as preventing COVID-19.