
Okay, I’m done with the things I was super busy with, but I’m still catching up. I’m hoping to pump out several posts in the next week or two.
Unexpected Side-effects
This paper reports that fertility in the US went up after the first year of the pandemic, the first time births per capita went up since the Great Recession.

My guess? People were bored and at home, so they had more sex.
Variants
I missed this, but this preprint (from Jan 2022!) says that Omicron was the result of a recombination between a BA.1 ancestor and B.35!
Vaccines
This article reports that NACI recommends that adults get a booster in the fall, and that the booster available will be a monovalent with recently-circulating strains (which I believe means XBB).
This preprint from USA found that mice vaccinated intranasally with NDV-HXP-S had really good immunity — including really good mucosal immunity. Reminder: NDV-HXP-S is the free-to-developing-countries vax made with really old technology (so is really really cheap) and uses a four-proline spike stabilization.
This press release from USA says that a Phase 1 trial in humans of NDV-HXP-S had good results, especially when delivered intranasally.
This preprint from UK found that people who were unvaccinated more likely to get diabetes after COVID-19 than vaccinated people. The unvaxxed were 4.86 times as likely to get a Type 2 diabetes diagnosis after a COVID-19 diagnosis than before (or without) a diagnosis. Vaccinated people were only 1.42 times as likely to get a Type 2 diabetes diagnosis as pre-COVID-19.
This paper from Italy found that COVID-19 vaccinations exacerbated psoriasis (although all patients recovered).
This paper from USA found that one dose of a bivalent booster wasn’t much better than a monovalent COVID Classic booster against Omicron, and theorize that it’s because of the immune system imprinting on COVID Classic. So they looked at people who got two bivalent boosters, and found that they still didn’t generate Omicron-specific antibodies. They think that a monovalent Omicron (like the XBB booster we’ll get in the fall) might help induce Omicron-specific antibodies.

COVID-Related Excess Death and Sickness
This report from the US Society of Actuaries found that the 2021 non-COVID deaths were ~15% higher than the baseline (pre-COVID) deaths. In 2022, non-COVID deaths were ~12% higher than baseline deaths. This might be undercounting of COVID deaths, or it might be that COVID-19 is hard on the body and damages it in ways that don’t show up immediately.
This paper found that for at least two years after COVID-19 infection, adults scored on cognitive tests like they were ten years older. The paper did say they only found effects in people who reported that they did not feel fully recovered, but that might be because people who had cognitive difficulties could tell that their brains weren’t working right.
This paper from Hong Kong (2023-08-16) found that COVID-19 put you at elevated risk for many illnesses, with adjusted hazard ratios of:
- multiple sclerosis: 2.66x;
- pernicious anemia: 1.72x;
- spondyloarthritis: 1.32x;
- rheumatoid arthritis: 1.29x;
- other autoimmune arthritis: 1.43x;
- psoriasis: 1.42x;
- pemphigoid (a skin disease): 2.39x;
- Graves’ disease: 1.30x;
- anti-phospholipid antibody syndrome 2.12x;
- immune mediated thrombocytopenia: 2.1x;
- vasculitis: 1.46x.
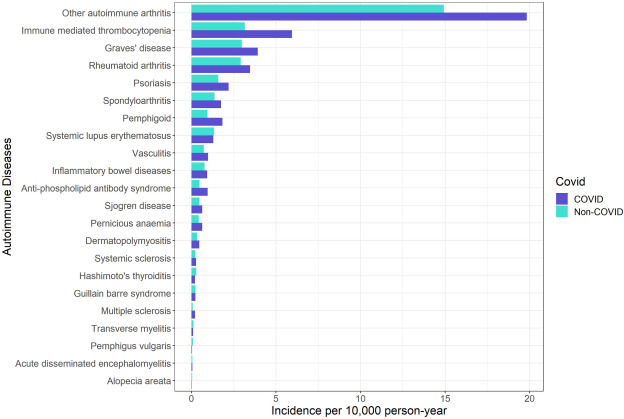
They also said that vaccination reduced the risk for most of the above ailments.
Long COVID
This paper from USA looks important. If I understand it correctly, it says that SARS-CoV-2 binds to pieces of the mitochondria and messes up the energy-production function and it triggers the innate immune system (which can cause cytokine storms). (See this blog post for a lay discussion of this work.) It’s even worse than that, because the virus hijacks the mitochondria so that instead of producing energy for the body, it produces more virus!
The mitochondria were still messed up after SARS-CoV-2 had cleared out.
This could explain why Long COVID patients are so tired: their bodies can’t make enough energy. (I’m hopeful this is what happens in ME/CFS also, that whatever treatment they find for Long COVID helps ME/CFS also.)
(This study looked at rodents and human cadavers, not living humans.)
This preprint (by a laaaarge international team) found an association between genetic variants in the FOXP4 gene was strongly associated with Long COVID. This is a BFD, but it might only be true for one type of Long COVID. I expect that we’ll find several different problems in Long COVID.
This preprint from UK found associations between a bunch of different genes are Long COVID.
This preprint from USA found that people who got Long COVID had higher maximum levels of SARS-CoV-2 RNA, infectious virus, and N-antigen, longer duration of viral shedding, and lower Spike-specific IgG levels within the first 10 days of the acute phase of illness. Interestingly, they did not have higher levels of various immune system markers. I assume that if Long COVID is in fact an autoimmune disease, they should have seen elevated levels of some of the immune system markers. (And this seems consistent with the previous paper, which says it’s mitochondria.)
This paper (from Oct 2021!) from UK suggests that Long COVID in women is related to low hormone levels. It notes that Long COVID affects more women than men; it notes that most female long haulers are around the age of menopause; it notes that 82% of the women reported worse symptoms in the region of their cycle where hormones are lowest.
This review article found that 16.2% of children had at least one symptom for at least three months after a COVID-19 infection.
This paper reports that 87% of the people who have Long COVID have internal tremors and vibrations.
Pathology
This paper found that people with a particular version of a particular gene (HLA-B*15:01) were highly likely to be asymptomatic when infected with COVID-19. This discovery might lead to better treatments!
This paper (from Nov 2021) from Italy found that men are 58% more likely to die from COVID-19 than women but only for men over 65. The rate is 2x for men in the 65 to 79 age group, yow!
This paper found that menopausal hormone therapy in women who had COVID-19 both reduced the risk of death and (especially) of long hospital stays.
This two-year study from Germany used wearable sensors to look at resting heart rate, daily physical activity, and sleep duration before and after COVID-19 infections and found that vaccinated people had smaller changes in their vital signs and reverted to pre-infection values faster than unvaccinated people.

This paper using data from 110 countries found that getting COVID-19 caused menstrual cycles to increase by 1.45 days (compared to their previous three cycles). Vaccination also increased the cycle length but by less — 1.14 days.
This paper from Denmark found that men who had had COVID had lower testosterone and fewer motile spermatozoa for at least six months post-infection.
This paper found that giving old hamsters drugs to kill off senescent cells — cells that have stopped dividing but which haven’t died yet — made COVID-19 infections less bad.
Transmission
This paper from Netherlands found that health care workers who admitted to picking their noses were 3.8 times more likely to catch COVID-19.
I can think of two reasons why this might be. The obvious reason is that virus on their hands would get smeared on their nasal membrane. But here’s another: people who have drier noses (more boogers, less snot) will be more uncomfortable and so more likely to pick their noses. The drier their nose, the more hospitable their nose is to viruses.
Unsolicited advice: I picked my nose way more when I was younger, before I learned to clean out my nose as part of my morning ablutions. If you clean out your nose in the shower, the mucous will be softer and more pliant, and your nose will be more comfortable for the rest of the day. You’re welcome.
This paper from China discussed an outbreak at an outdoors night market in Qingkou. They identified three people (all from the same family) who were at the night market for 1 hr 4 min and infected 131 people while they were there.
Now, I wonder if there was another infection vector running around, as there were a few infected people who left the night market before the three family members arrived. But regardless, that’s an awful lot of spread for being outdoors.
I tend to think that “outdoors is magic”, and that I’m pretty safe from COVID-19 outdoors. The night market clearly wasn’t, but there were some things were not in its favour:
- It was night. That means there was no UV.
- It was really really crowded.
- They were outdoors, yes, but part of the night market took place on a street, which meant that airflow was more constrained than at, say, Stanley Park.
- There was very little wind that night.
So I guess I need to be a little more careful at night.
Testing
This paper from USA says they have developed a COVID-19 breathalyzer which can tell with high accuracy if someone has COVID-19 or not.
This article from the COVID-19 Immunity Task Force says that the seroprevalence of COVID-19 nucleocapsid antibodies (i.e. ones you get from infections, not vaccinations) actually dropped slightly from April to June, to 77.8%. They say that might be from basically measurement noise or from antibodies waning. I didn’t know antibodies waned so much.