
I have been busy for the past eight weeks, so am behind on my COVID-19 research. I’m still not caught up, and there’s no real reason to publish today except for f it, I need to publish sometime. So here you go!
COVID-Related Excess Death and Sickness
This paper using data from Hong Kong and the UK calculated the increased risk of various things after the acute phase of COVID-19 ended for 17 to 28 months. They found:
- 1.82x risk of heart failure;
- 1.31x risk of atrial fibrillation;
- 1.32x risk of coronary artery disease;
- 1.74x risk of deep vein thrombosis;
- 1.61x risk of chronic pulmonary disease;
- 1.89x risk of acute respiratory distress syndrome;
- 3.91x risk of interstitial lung disease;
- 2.32x risk of seizure;
- 1.65x risk of anxiety disorder;
- 1.52x risk of PTSD;
- 1.76x risk of end-stage renal disease;
- 2.14x risk of acute kidney injury;
- 1.42x risk of pancreatitis;
- 2.86x risk of cardiovascular mortality;
- 4.16x risk of all-cause cardiovascular mortality. (I.e. you are four times as likely to have a cardiovascular issue which kills you in the ~2 years after you have COVID-19.)
In this paper from Brazil, they found that a quarter of people who had had mild COVID-19 infections (mostly mild) had unusual difficulty in using visual and spatial information to guide complex behaviors (like drawing, assembling objects or organizing multiple pieces of a more sophisticated stimuli).
I am not the only person who wonders if this could be related to the increase in traffic accidents since the pandemic started. This is not the first paper to connect COVID-19 with accidents: See for example:
This paper from Canada from Feb 2023 finding that unvaccinated people were 48% more likely to get in traffic accidents than vaccinated people (after adjusting for age, sex, home location, socioeconomic status, and medical diagnoses).

This report from the US National Highway Traffic Safety Administration found that traffic fatalities increased hugely post-lockdowns over pre-pandemic levels.

This article from France from now reports that while the total number of accidents in 2021 was about the same as pre-pandemic, there were big jumps in the number of motorway fatalities (up by 12% over pre-pandemic) and cyclist deaths (up 30%).
This article reports that traffic fatalities in 2022 were up at least 10% over 2019 in the Netherlands.
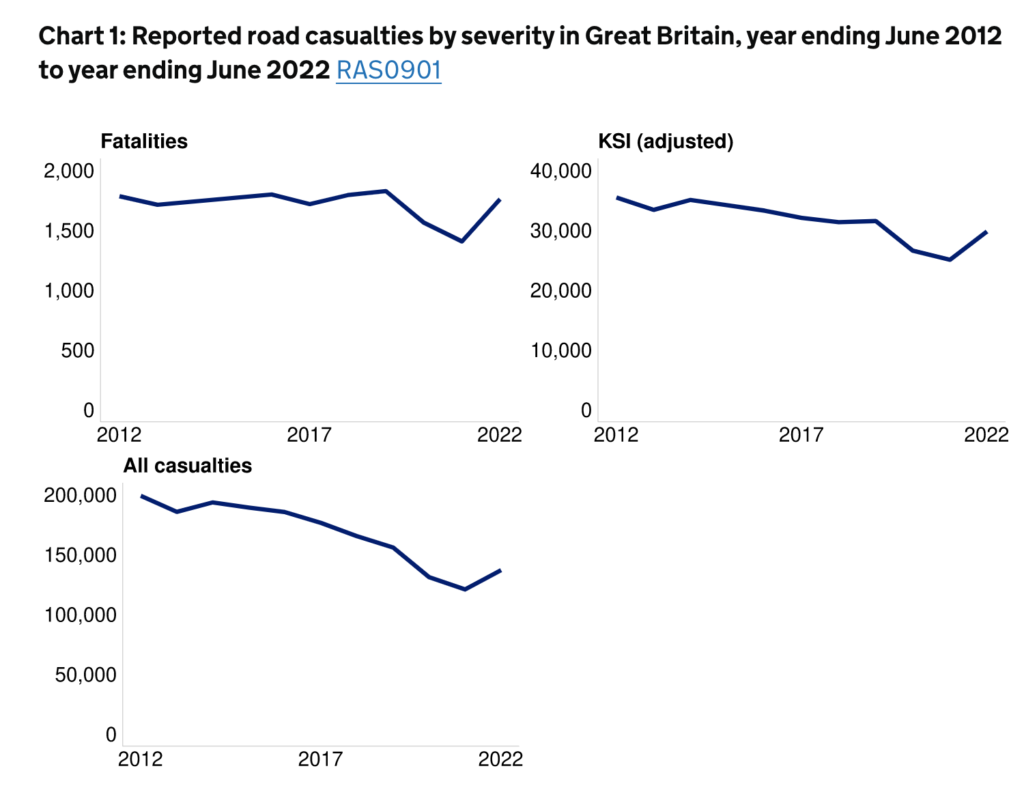
However, this report from the UK government from Nov 2022 says that traffic accidents were down in the UK compared to pre-pandemic.
This paper from USA found that people who had had COVID-19 infections were about three times as likely to have a low ratio of stress myocardial blood flow to resting blood flow. Yeah, okay, that’s a kind of strange measure, but basically it means they can’t boost their blood flow as much when they need it.
Long COVID
This small study preprint from Spain found that the vagus nerve was… funny in people with Long COVID who had symptoms suggesting vagus nerve dysfunction compared to controls. Digging through all the technical terms, I think their vagus nerves were thinner and fattier. If I understand correctly, the Long COVID patients also had more:
- signs of chronic overinflation of their lungs;
- difficulty swallowing (poorer esophageal peristalsis);
- gastroesophageal reflux (GERD);
- hiatal hernias (where the stomach pushes through the diaphram muscles);
- difficulty breathing in (reduced maximal inspiratory pressure).
All of these apparently are signs of the vagus nerve/autonomic nervous system not working as well.
This paper from Australia found that SARS-CoV-2 caused cells in the brain to fuse together, which impaired neuronal activity. The same mechanism which the spike uses to connect to the ACE2 receptor to get inside the cell seems to also let/help the ACE2 receptors to connect to each other on two neighbouring cells. Ewww.
This paper from Switzerland found that 22.9% of people who had COVID-19 infections were not fully recovered in six months. The excess risk for various individual symptoms was:
- altered taste or smell – 9.8%
- post-exertional malaise – 9.4%
- fatigue – 5.4%
- shortness of breath – 7.8%
- reduced concentration – 8.3%
- reduced memory – 5.7%
This preprint from all over the world found that vaccinations reduced the risk of Long COVID. How much varied by country, ranging from 16% to 45%.
Vaccines
This article says that the US FDA asked for the fall vaccines to be monovalent shots based on XBB (preferably XBB 1.5). That probably means Canada will get monovalent XBB vax also.
This paper from Mexico reports on a Phase 1 trial of NDV-HXP-S.
To remind you of why I am excited about NDV-HXP-S:
- NDV-HXP-S uses a Newcastle virus, which is something most people don’t have any immune defences against, unlike adenoviruses (which most viral vector vaccines use).
- Its spike protein is stabilized with the 6-proline modification, unlike Moderna and Pfizer, which use the 2-proline modification. The stabilizations keep the spike from flopping into the “open” position, and the 6-proline modification does a better job than the 2-proline modification. This means that a higher percentage of the vaccine particle are in the useful “closed” position, so you need less of it.
- It’s made using very old technology (which includes chicken eggs), so it is reeeeeallly cheap.
- The NDV-HXP-S license is free to developing countries. Mexico, Thailand, Brazil, and Vietnam are all making versions.
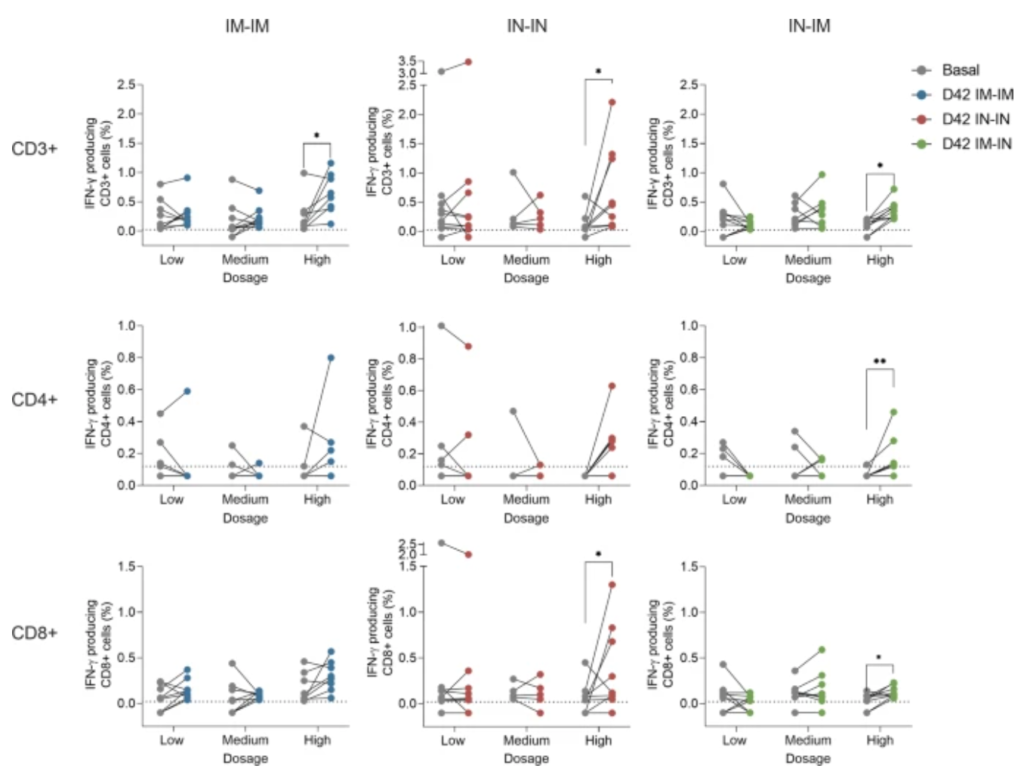
The Mexico study was mostly to look at safety, and the vaccine looks very safe, as expected. They also did a little bit of looking at delivery, both where to inject and how much. They tested low/medium/high doses in intramuscular first and intramuscular second (IM-IM), intranasal-intranasal (IN-IN), and intranasal-intramuscular (IN-IM).
I was disappointed that the levels of general spike antibodies in blood were much higher for IM-IM than either of the IN versions. For example:

But I guess this isn’t really surprising, as the whole deal with intranasal is that it should elicit antibodies in the mucous membranes, not the blood. However, the IN vaccinations did a lot better at eliciting the specific antibodies that gum up the Receptor Binding Domain (i.e. prevent the virus from attaching to the ACE2 receptor):

The mixed vaccinations did clearly do well at eliciting responses from T cells, especially at high doses:
They did not quantify the intranasal antibodies because it’s hard, there’s no standard for it, and that’s not the main purpose of a Phase 1 study. We’ll have to wait for that. (They’ve already started a Phase 2/3 study, so hopefully I uh I mean we won’t have to wait long.)
Note: I believe data collection portion of the study went from May 20, 2021 (Alpha regime) through August 21, 2022 (Omicron regime), while the vaccine is based off of COVID Classic. That means that the vaccine might look crappier than it would if/when it gets adjusted for the current strain.
Another vaccine called CORAL from Gritstone Bio in USA has completed a Phase 1 trial of GRT-R910 as a booster in UK (based on COVID Classic) and another Phase 1 trial of GRT-R914 with vaccinated and unvaccinated people in South Africa (based on Beta and Omicron) with good news. They found lots of antibodies to all the strains they checked, even after six months!

UC-Irvine has a vaccine which presents the immune system with epitopes (little pieces) of the spike which don’t change much from strain to strain. This preprint discusses intramuscular injection in mice; this preprint discusses intranasal vaccination in mice. Both did a good job of protecting the mice from a number of different VOCs.
Transmission
This paper from the USA found that between October 2019 and October 2022, 70% of household infections came from a child, and that household transmission rates dropped when school was not in session.
Caveats: they used smart thermometers to determine when there was a COVID-19 infection. If people caught something else (which mostly they didn’t from March 2020 until late October 2022), or if they got sick and didn’t have a fever, those could throw the results off.
This paper from UK found that — surprise surprise — hospital-acquired COVID-19 infections went up when they stopped testing incoming patients. It went up from 0.99 per thousand to 1.64 per thousand in England and from 1.00 per thousand to 1.39 per thousand in Scotland.
There was a controversial study in the UK where they deliberately infected some healthy young adults and studied the hell out of them. This paper found:
- They found viral RNA from about half of the patients in breath samples, mask samples, hand swabs, and surface swabs.
- Breath emissions more strongly with nasal measurements than throat measurements.
- Two patients emitted 86% of the airborne virus. (!!) These were not the patients who were sickest.
- The majority of airborne virus collected was released on 3 days.
- Very few breath emissions occurred before the first reported symptom (7%) and hardly any before the first positive lateral flow antigen test (2%). (!!)
I’ve taken a look at the data, and the best conclusion I have is.. boy, there is a huge amount of variability. While it seems like some people are not that contagious (Participants 12 and 17), while other people are contagious for a long time.
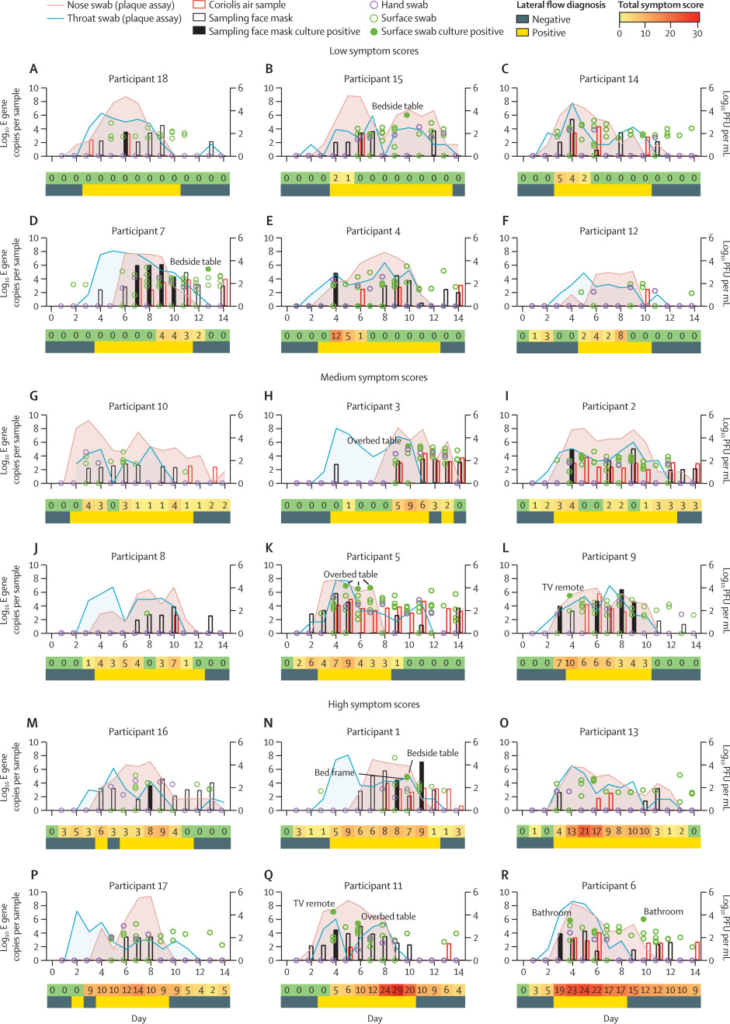
For example, Patient #7 had low symptoms and high levels of culturable virus in their masks on the TENTH day after exposure.
Pathology
This paper from USA found that women who have the best sleep habits before they got infected are 30% less likely to get Long COVID than women with the worst sleep habits.
This paper from Netherlands found that people with inflammatory rheumatic disease were 2.52 times as likely to get Long COVID after COVID-19 infections than people without inflammatory rheumatic disease.