
Long COVID
This paper from the UK says that people who have had COVID-19 infections are five times as likely to die in the 18 months post-infection than controls.
This paper says that people who were unvaccinated were more likely to have lingering illness for at 28 to 89 days than the vaccinated, and that the worse the COVID-19 case was, the more likely they were to have a lingering case: unvaccinated moderate cases were 80% more likely to linger and unvaccinated severe cases were 125% more likely to linger than vaccinated patients. People who were unvaccinated, got COVID-19, then got vaccinated were 41% less likely to have symptoms at six months than those who never got vaccinated.
They also found that people who had COVID were more likely to have other problems at six months than those who did not:
- 2x chance of pulmonary problems;
- 1.46x chance of diabetes;
- 1.29x chance of neurological problems;
- 1.28x chance of mental health problems.
This paper from the USA says that the risk of death in the first year post-COVID-19-infection is higher than in controls for various types of death but not cardiovascular deaths.
- all causes death: 2.82x risk;
- arterial thrombotic events: 2.26x risk;
- venous thromboembolism: 9.33x risk;
- serious cardiac arrhythmias: 3.37x risk.
(NB: I thought that clot deaths were “cardiovascular deaths”, so I’m not sure what CV actually means in this article. Heart attacks?)
Pathology
This paper (from May 2022) from the USA says that RNA of SARS-CoV-2 is found in the bloodstream (“RNAemia”) of many but not all COVID-19 patients, and that the chance of finding it in the blood increases with severity:
- ICU patients: 100% chance of finding SARS-CoV-2 in plasma;
- hospitalized non-ICU: 52.6% chance;
- non-hospitalized: 11.1% chance.
This was not surprising; there have been other papers (like this one from July 2022 and this one from March 2022) which link outcome to RNAemia. However, it wasn’t clear if those were just fragments of viruses or if they were culturable (which would be viremia and not just RNAemia). I couldn’t follow the details, but the authors concluded that the RNA that they found was from actual virus particles, not just pieces.
(I was surprised that not all COVID patients had SARS-CoV-2 virions in the blood; I had assumed that SARS-CoV-2 was always in the blood!)
Vaccines
This article reports that the US CDC found a possibility of increased strokes in people over 65 for people who got the Pfizer bivalent vax, when looking at data from states. They looked at a shitton of other data sources, and couldn’t see a problem in those other sources. They are still examining, but it’s probably a case of hypervigilance.
From this tweet, here’s an updated table summarizing the effectiveness of bivalent boosters:

This paper from the USA found that three doses of the original mRNA vaccines wasn’t effective against XBB.1.5 (dark greenish in the figures below), but that a booster of bivalent BA.5 was effective.

If someone tells you that vaccines are causing sudden unexplained deaths, point them at this Substack post‘s graph (from UK data):

What about how way more young people are dying now than used to be? That same post has you covered, this time with USA data:
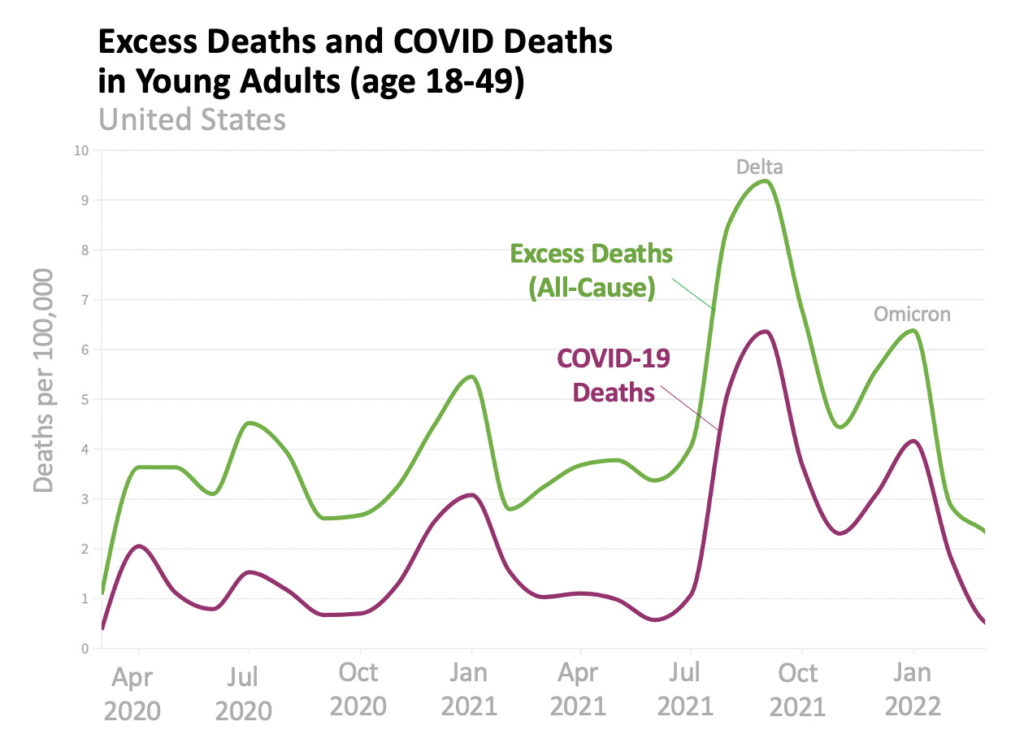
The posts speculates that a lot of excess deaths which were not attributed to COVID-19 were from secondary effects — heart attacks from COVID-weakend hearts, drug overdoses from lonely people, etc.
If you look just at circulatory system attacks in young people in the USA, you can see that the rate was going down pre-pandemic, then spiked post-COVID but pre-vax, and then slowed down again after vaxes showed up:

It’s a good post.
This paper discusses why it’s hard to get vaccines which give persistent immunity for common colds / flu / COVID, while vaccines for diseases like measles or mumps give lifetime immunity. The theory is that the diseases that vaccines give sterilizing immunity to are ones which get into the blood, where they interact with lots of different parts of the body’s immune system, giving all the different immune system pieces a chance to train defences. (They also have a very slow incubation period, unlike respiratory infections.)
The paper also says that humans have evolved some tolerance for respiratory infections. Basically, we inhale so much crud that if we called out the big guns every time we got an infection, we’d cause damage to our own cells.
The bottom line of this paper is: developing a vax which gives sterilizing immunity is going to be hard. 🙁
Treatments
This review-article preprint from the USA says that convalescent plasma reduced mortality by about ten to twenty percent. (I was surprised, because there had been a lot of studies early in the pandemic which said that convalescent plasma did not help.) It also found that there were better results with earlier treatment and with plasma that higher antibody levels.
Recommended Reading
If you are into Long COVID research, this review article has lots of detail about what they know about the pathology. This review article looks at what treatments have been tried and how well they do.
This article talks about Long COVID treatments.