
Mitigation Measures
This article reports that a poll found that 69% of Canadians would either support or “somewhat support” a mask mandate for indoor public spaces if there are rising case counts. In BC, 72% said they supported or “somewhat supported” such a mandate.
Long COVID
This paper from Germany lays at least part of the blame for brain fog at the feet of microglia (which are kind of the brain’s janitorial service). They also found elevated levels of CCL11 in people with brain fog, which could be useful as a biomarker.
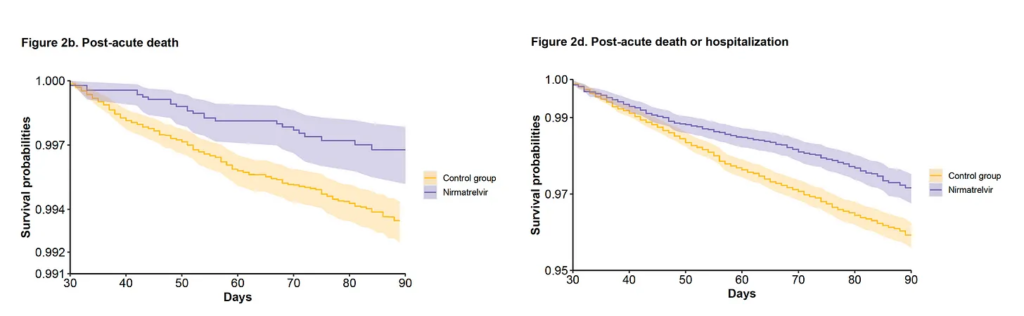
This big study from the USA Department of Veteran’s Affairs (which, alas, means mostly men) found a 26% decrease in Long COVID among people who had been given Paxlovid.
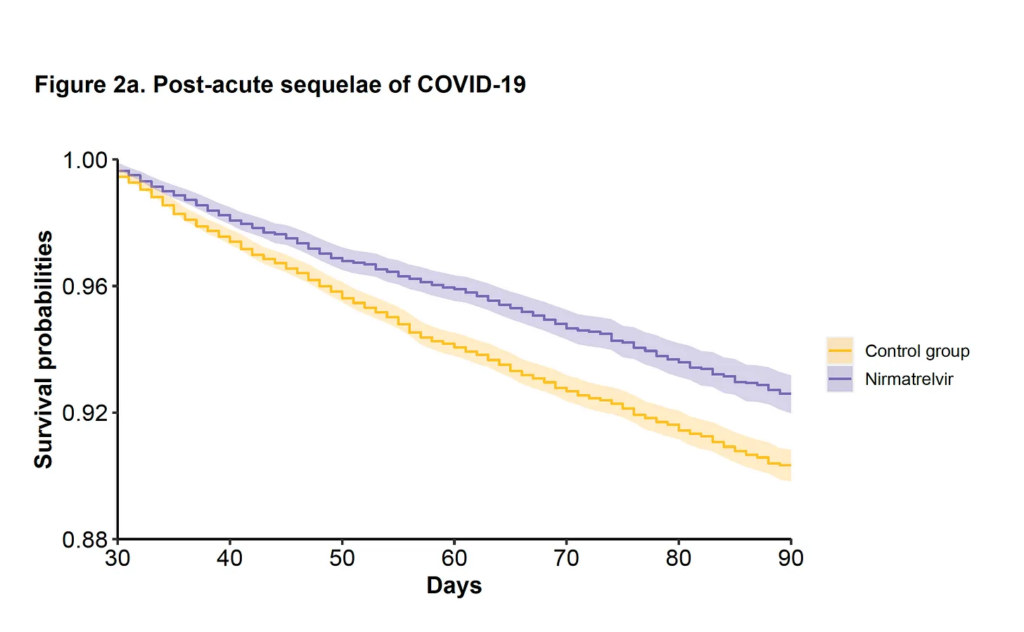
there was no difference given vaccination status, prior infection, unvaccinated status, co-morbidities, or gender (though it was heavily skewed male).
Something that I find really interesting is that Paxlovid drops all-causes mortality even after the acute phase is over. This is another reminder that COVID-19 can kill you even after you have “recovered”.
Finally! There’s going to be a big random clinical trial of Paxlovid for Long COVID patients.
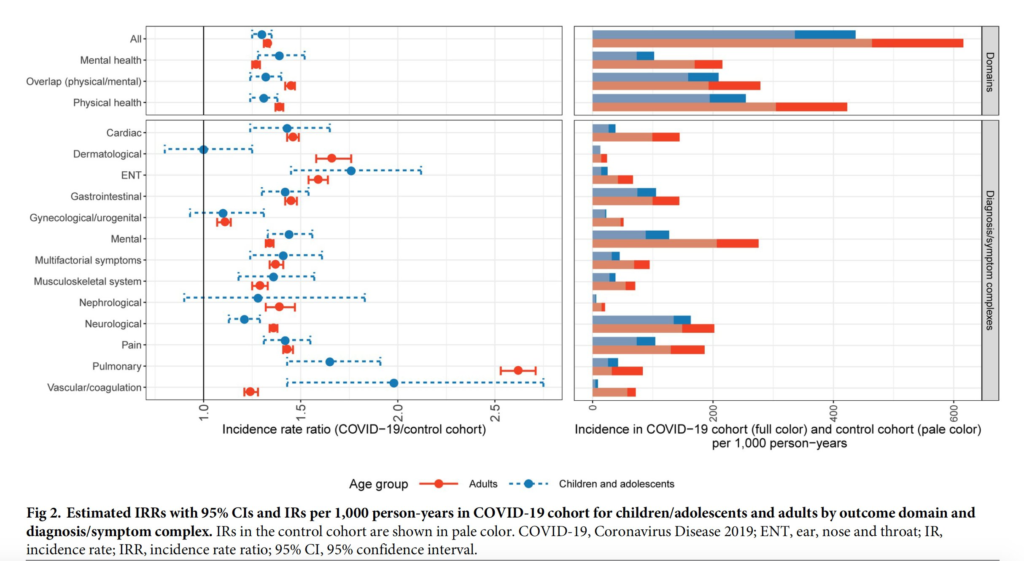
This big study from Germany says that, surprise, surprise, kids can get Long COVID too.
This paper from the USA says that people who had had major life stressors (like loss of job, loss of spouse) were significantly more likely to get Long COVID. Life is unfair.
This preprint from the USA found that, in a pilot, 8 of 12 Long COVID patients got better after getting non-invasive electrical stimulation of their vagus nerve.
Testing
This paper found that more COVID-19 testing at two university campuses led to riskier behaviour. Interestingly, they said that women seemed to drive the behaviour because they take the risks more seriously (in general).
I know that I was skeptical of frequent testing as a way to mitigate spread in BC because tests were everywhere in the UK relatively early on in the pandemic, and it didn’t seem to help them.
Mitigation Measures
This study from the USA looked at schools which did and did not lift mask mandates. Schools which did lift mask mandates had an additional 44.9 more COVID-19 cases per 1000 students and staff during the 15 weeks after the statewide masking policy was rescinded than those which did not.

Vaccines
So are the bivalent boosters really any better than the Classic boosters? There’s conflicting data — evaluations which use pseudoviruses say no, but evaluations which use actual live viruses say yes, some. Pfizer recently announced data in the latter camp. They are certainly no worse; they area also not huuugely better. A little better.
Novavax Inc issued a press release which said that an experimental bivalent version wasn’t any better (or worse) than Novavax Classic.
This study from Israel during the BA.1/BA.2 time period found that four doses of Pfizer were better than three, but that the fourth dose’s antibodies waned faster than the third dose’s: the fourth dose waned to third-dose-leve in 13 weeks (and then stabilized).
This paper says that the antibodies which are most effective are the ones that glom onto the prefusion (“closed” configuration) spike, especially the S1 subunit. This surprised me, as one reason I had heard for Novavax’ surprisingly broad protection is that it does a better job showing the S2 subunit to the immune system than other vaccines. But then I saw that what they used to test effectiveness was the Wuhan strain! It’s not a big surprise that vaccines which elicited antibodies to the Wuhan S1 protein would do well. Unfortunately, S1 is where most of the VOC’s mutations are! It is easy for me to imagine that antibodies targeting the Wuhan S1 would not do well against the BA.5 S1s.
I missed this paper from Moderna from October, but they tried an experimental vax which only had two (important) pieces of the spike protein instead of the full spike protein. They found that 10µg of the experimental vax worked about as well as 100µg of the Moderna Classic vax.
Pathology
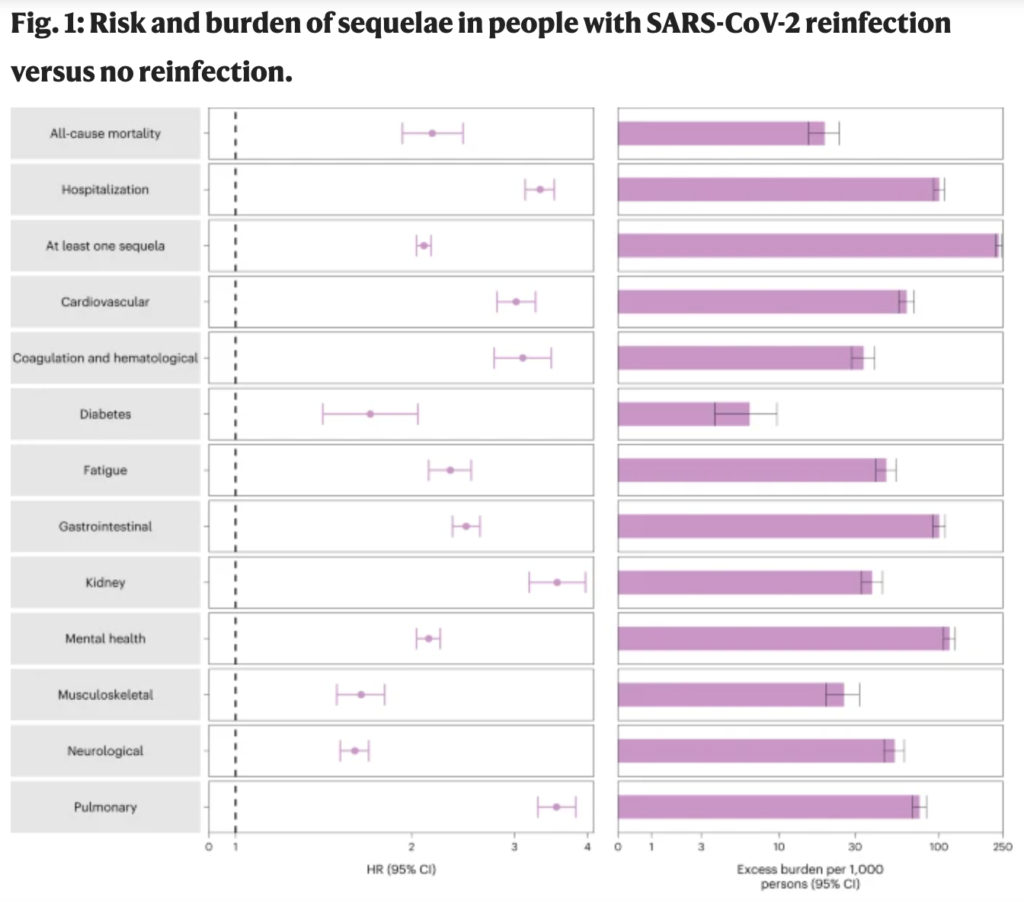
This big study from the USA found that reinfections are (surprise!) bad. A reinfection more than doubled the risk of death (over people who just had one infection), more than tripled the risk of hospitalization, and Long COVID. The risks were biggest during the acute phase, but there was risk which lingered for at least six months. Interestingly, vaccination didn’t appear to reduce the risk of Long COVID for people who got reinfected.
This article (about this paper from the USA) is wild. Apparently a fair number of people who have been put on a ventilator and anesthetized (because that’s what you do when you vent someone), when they recover enough to come off the vents and the anesthetic, they just… don’t wake up for a long time, like two or three weeks!
Treatments
This paper suggests that melatonin might be useful for treating Long COVID. (It’s pure speculation as far as I can tell, but intriguing.)
Recommended Reading
This article explores the (somewhat fringe) idea that COVID-19 can trash your immune system. I am skeptical because we have not seen measles outbreaks (if COVID-19 erases your immune system’s history like chemo/marrow transplants do) or unusual numbers of pneumocystis pneumonia (if COVID-19 destroys the immune system’s ability to fight like AIDS does ). I sort of feel like if millions of people’s immune systems were getting trashed, we’d be seeing lots of cases of either measles or pneumocystis pneumonia. However, there are some interesting points in the article, and I am not a doctor, so could be wrong.
This article talks about a shift from “how many doses” to “how recent was your last dose”.
This article talks about how the pandemic changed Canadians’ relationship to food shopping/cooking
This article talks about why so many kids are getting sick now. (Spoiler: because they didn’t get sick before.)