
Transmission
Here’s another preprint (from the UK) which says that the “you don’t have to isolate longer than five days” guidance is bullshit. It says that the median person was infectious — even if asymptomatic — for 7 to ten days.

This paper from the USA found that while adults who were not exposed to kids age 0-5 y/o were 15% less likely to catch COVID-19 than people with exposure to kids 0-5 years old, if they caught it, they were ~50% more likely than their matched little-kid-exposed cohort. The low-kiddie-contact cohort was also 76% more likely to go into the ICU than the high-kiddie-contact cohort. The authors speculate that this might because the little ones give adults more exposure to the “common cold” coronaviruses, which could give some protection against COVID-19.
On the other hand, this paper from the USA says that people with children in the home in multi-unit dwellings (i.e. apartment buildings unless I am badly mistaken) had 10.5x the risk of going to the hospital than those with no kids. For people with children in their home in single-family homes, the risk of hospitalization was 2.2x. (Note: “children” here is anybody under 18, so a slightly different age group.)
In the multi-family dwellings, the risk of hospitalization was 2.5x higher for people living in a household of more than four people than for people living alone; the risk was 0.8x for single people living in single-unit dwellings than for a single living in a multi-unit dwelling.
This preprint from Italy found that ventilation ranging from 10 to 14 liters per second per student reduced the likelihood of infection for students by 80% compared with a classroom with only natural ventilation.
This preprint from Portugal (where 98% of the population is “fully vaxxed”) found that previous infections gave good protection against BA.5 compared to the uninfected group that varied by which variant they were infected with:
- COVID Classic 52.9%;
- Alpha: 54.9%;
- Delta: 62.3%;
- BA.1/BA.2: 80.0%
Note that the earlier infections were also, well, earlier in time, so maybe the protection from infection wanes over time like vaccines do?
Variants
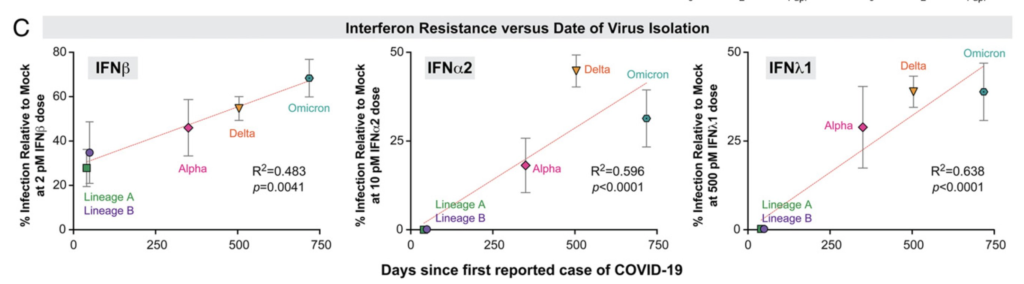
This paper says that newer variants evade our innate immune system more than COVID Classic did. In other words, it’s not just vaccine evasiveness.
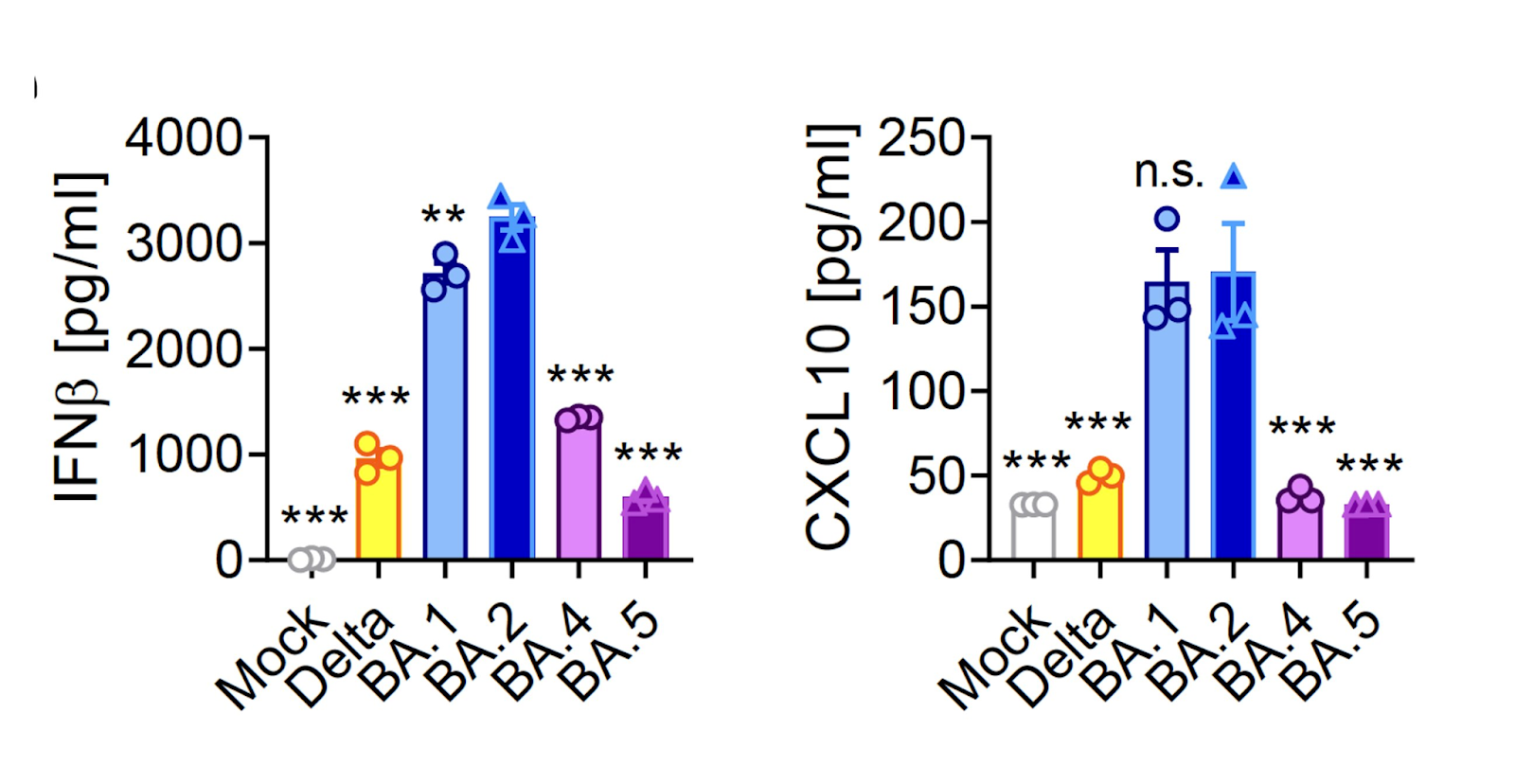
This preprint from the UK says that BA.4/5 evades the innate immune system more than previous variants:
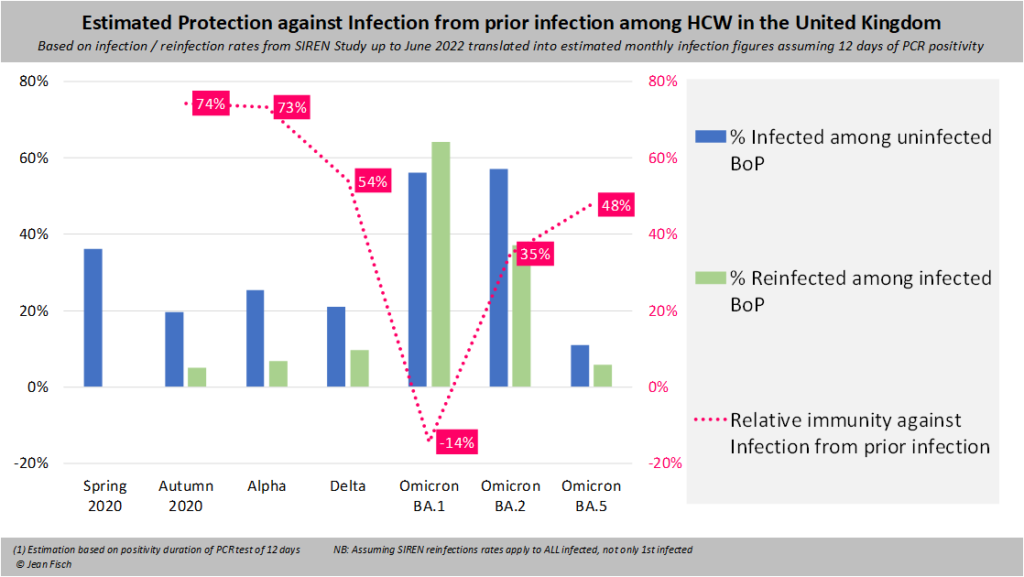
This twitter thread says that the amount of protection which a previous infection gave varied depending on the variant:
Vaccines
Buried at the end of this article is something which says that parents can start booking appointments for kids under 2 can get vaccinated starting 2 August.
This preprint from Portugal (which has had a baaaaad BA.5 wave) found that vaccines prevented infection just as well against BA.2 and BA.5. However:
- the risk of reinfection was 44% higher for BA.5 than it was for BA.2 regardless of the vaccine status;
- the booster protection against hospitalization was significantly higher for BA.2 than for BA.5 (93% vs. 77%);
- the booster protection against death was significantly higher for BA.2 than for BA.5 (94% vs. 88%).
This correspondence from China says that a third dose doesn’t help unless you’ve never gotten COVID. (It found that if you had two doses plus an infection, you’ve got more protection than from three doses alone.)

This paper says that a shitton of people had menstrual irregularities after vaccination. Of people with regular menstrual cycles, 42% bled more heavily than normally. (44% reported no change, and I don’t know wth the other 14% said.) For those who do not menstruate regularly, a lot had breakthrough bleeding. including:
- 71% of those with period-blocking contraceptives;
- 66% of those post-menopause;
- 39% on gender-affirming hormones.
The changes only lasted one cycle.
Long COVID
This paper says that the Long COVID symptoms that people who have had COVID-19 are most at increased risk (compared to people without COVID-19) are:
- loss of smell (6.49x risk);
- hair loss (~4x risk);
- sneezing (2.77x risk);
- ejaculation difficulty (2.63x risk);
- reduced libido (2.23x risk);
- shortness of breath at rest (2.2x risk);
- fatigue (1.92x risk);
- pleuritic (i.e. worse when you breathe, cough, or sneeze) chest pain (1.86x risk);
- hoarse voice (1.78x risk);
- fever (1.75x risk)
This preprint tells of one Long COVID patient who saw a significant reduction in symptoms when on Paxlovid and/or tocilizumab (an arthritis drug).
This review article says that 5.6% of COVID-19 patients lose their sense of smell and 4.4% lose their sense of taste. 95.7% of them recovered their sense of smell and 98% recovered their sense of taste get it back within six months.
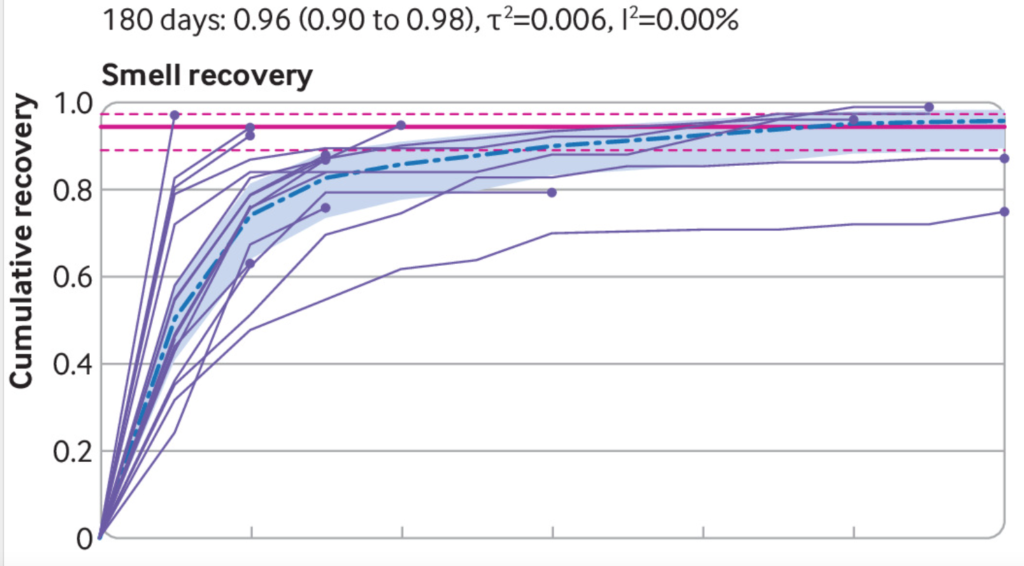
Women were about half as likely to get their smell/taste back.
Pathology
This article reports that scientists think they have cracked the pediatric hepatitis outbreak (see preprint). It appears that there’s an adenovirus which is a dependovirus (yes, that’s a word! — it means that it depends on another virus being present to replicate) called AAV2. If you add AAV2 and a helper virus and a particular genetic variant (found in 16% of Scots, so not all that rare), THEN you can get pediatric hepatitis. So it looks like pediatric hepatitis is not linked to COVID-19. (Except that maybe the COVID measures meant that a bunch of childhood respiratory diseases kind of got saved up and all hit at once, which increased the chances of AAV2 having a helper virus around?)
This paper says that people who smoke have somewhat higher risks of bad outcomes from COVID-19. Smokers had this much higher risk than non-smokers:
- 41% higher risk of death;
- 15% higher risk of mechanical ventilation;
- 27% higher risk of major adverse cardiovascular events.