
NOTE: I had been grabbing the number of tests from the wrong place on the BC CDC dashboard, which meant that my positivity numbers were wrong. I’ll go back and fix blog posts retroactively, but among the charts below is a rolling 7-day average of positivity from the BC CDC dashboard.
Transmission
I’ve gotten some pushback on yesterday’s BC COVID-19 Modelling Group’s numbers.
- It’s their analysis, not mine.
- I picked the 50K number off of the graph which they thought was most likely. I do have to apologize, it looks like I didn’t eyeball properly, really it’s more like 80K.

Yesterday, I carefully did not say if I endorsed their numbers or not. I wasn’t sure. The numbers sure seemed hella high, but they used a more careful analysis based on the case rate of over-70s, which looked perfectly defensible. (Watch their video to see how they come to their conclusions.) The fact that I didn’t like it and that it didn’t jibe with what I had been seeing was not a reason to say that it was wrong. Maybe I was wrong?
A quick review of why I had thought the cases were falling:
- The seven-day average of the reported case rate is falling. Yes, the reported case rate is bogus, but it’s been bogus in the same way since they changed who they would test, which I believe was around Christmas, and certainly no later than New Year’s Eve.
- The testing rate and positivity rate have both gone down since their peak (see below). (Yes, the seven-day rolling average of the positivity rate went up a little recently, but overall it is down from its peak.) In situations where the case rate is constant, the testing rate and the positivity rate are inversely correlated. For them to both be going down is a strong signal that the actual case rate is going down.
- Dr. Henry said on 2022-01-14 that they believed the cases peaked recently. Granted, it is possible that they are wrong, but they do have access to the best data and strong incentive to get it right.
- Other jurisdictions around the world have seen fast-up, fast-down case rises and falls. Granted, every jurisdiction has a different pandemic because of different demographics, different vax/booster rates, different vax brand mixes, different measures, and different compliance. However, BC’s got a really good vax rate, non-zero mitigation measures, and a pretty compliant population (yay!). It is emotionally difficult for me to think that we are in worse shape than the US and UK.
- The wastewater surveillance shows that levels of COVID-19 started dropping in early January (see figure below). However, the BC COVID Modelling points out that we got a lot of rain in early January, and the levels are meaningless unless they are normalized to rainfall. That sounds reasonable at first, but this morning I realized something: STORM SEWERS AND SANITARY SEWERS ARE SEPARATE; IT DOES NOT RAIN IN MY TOILET. The amount of human waste produced is relatively constant. THE WASTEWATER SURVEILLANCE DOES NOT NEED TO BE NORMALIZED TO RAINFALL.



I now believe the wastewater surveillance is absolutely the most rock-solid evidence of all of the data points. I now believe that the BC COVID-19 Modelling Group got it wrong.
This article reports that the province has explicitly changed how it handles cases in long-term care homes. It used to be that they declared an outbreak if there was one case among staff or residents; now it’s only if they can’t contain the outbreak, whatever that means.
I want you to stop and think about what it thus means that there are ~60 LTCH outbreaks right now. 😬
Mitigation Measures
There are articles like this one reporting that the guidance has changed that if you get sick but haven’t gotten tested, then you don’t have to isolate at all. I don’t think that’s exactly what the province says, but it is true that the province is incentivizing not getting tested. The province says that if you get sick, stay home until you feel better: “If you have mild symptoms and do not need a COVID-19 test, stay home until you feel well enough to return to your regular activities.” If you test positive, you are required to isolate for five days if you are vaccinated and ten days if not vaccinated, regardless of your symptoms. I don’t get it.
Press Briefing
The briefing opened with a discussion of risk factors. The Case Hospitalization Rate for Omicron is 1.25%, while back in October, it was 6.2%. In other words, Omicron’s CHR is one-fifth that of Delta. That’s good, except that the max confirmed case rate during January is almost 6x what the max confirmed case rate was in October… and it is likely that the actual case rate in January is a significantly higher multiplier over confirmed than it was in October. (To be fair, the time spent in hospital with Omicron is half of the time spent for Delta.)

They also showed various risk factors:


Dr. Henry talked about contact tracing. She said that contact tracing works well when the disease has:
- A long incubation period (so you have enough time to find the contacts);
- Low infectiousness (so that the contact tracers aren’t overwhelmed);
- Effective treatments for the disease (so you can do something about it).
COVID-19 was like this in the early days, but its incubation period got shorter and infectiousness got higher, so contact tracing is basically pretty useless now. (<- Not her exact words.) Dr.H said we need to shift to vaccination, self-mangement, and testing for people in high-risk groups, and that’s what we have been doing.
Yes, this is a shift, she says. We cannot eliminate all risk, we’re going to have live with this for years to come. What we can do, she says, is use all our layers of protection to keep our workplaces, healthcare, and schools running and safely as possible. She says now we need to all — all of us — assume that we have been in contact with someone with COVID-19, check our symptoms daily, stay home if we are feeling unwell, and Do All The Things. She said that if we been exposed, it’s not necessary to isolate because fuckit, everybody’s got it now (<- not an exact quote, but I think that’s the gist of it).
Use the BC CDC symptom checker to determine if you need to get tested — if your symptoms are severe enough or if you are in a high-risk group.
She talked about the balance between keeping LTCH residents safe and also giving them the quality of life they need, so they are changing how they handle outbreaks. But she didn’t say how.
She acknowledged that we are changing a lot and that change is hard.
Dix gave updates on RATs: we’ve gotten received almost 6M RATs to date, and have deployed ~3.9M already, leaving about 2.1M supply. (About 1.1M arrived since Monday.) About .5M of the recent shipment are not suitable for take-away. ~150K will go to acute-care facilities, ~192K to testing sites, ~150K to K-12 education system, ~237K to businesses, and a bunch to LTCH screening programs.
Dix said they expect to receive another 15.7M from the federal government by the end of February.
Jan 17-19, 7950 HCW called in sick (not all from COVID-19). This is better, down from 11K Jan 10-12.
Dix went through the further reductions in services due to increased hospitalizations.
Dix gave the numbers of scheduled surgeries which have been postponed.
Q&A
Reminder: I paraphrase heavily and snarkily. Dix and Henry do not use the spicy language that I do.
Q: It seems like you went from non-edemic mode to endemic mode in just a few days, even though our hospitals are still getting slammed, wtf? A: That is not correct, it is clearly not endemic. What we are doing is adjusting to the new variant. Omicron has a shorter incubation period and milder and vax is not 100% effective, so we have to deal with the variant as it is. It’s not my choice that Omicron is causing more illness in HCW and other workers, so we have to Do All The Things.
Q: Other jurisdictions are saying/doing different things in other jurisdictions, especially around isolation, like Dr. Tam says your symptoms can last for more than ten days. A: Absolutely your symptoms can last for more than ten days, but your risk of transmitting goes down after five or six days. We are trying to balance the risk of not having HCW with having sick HCW. Across the country we are dealing with different proportions of Delta to Omicron; I watch PEI because that’s where I’m from, and this is their first wave, so they don’t have a lot of the mitigations like COVID safety plans in place.
Q: Why was there this confusion where unvaxxed people only had to isolate for five days and then it went back to ten, wtf? A: We fucked up. My staff is tired and stressed and a lot of people are out sick.(<- not a direct quote)
Q: You said today that Omicron is not mild but today you said it was milder. A: Arg, “mild” is such an awful word. It’s important to not just let it rip, we still need to Do The Things to protect the vulnerable, but I’m trying to convey that for many people it is less severe, but it is not an innocuous illness.
Dix: On an individual basis, it is less severe but there are a shitton more individual cases, which causes big problems. We are doing a lot, especially giving a shitton of boosters and doing a lot of RATs. Also note that we started preparing our healthcare system before Xmas for this surge. And it’s been months since I’ve seen someone in a grocery store without a mask.
Q: Minister Dix, Fraser Health says that non-COVID patients can be put in rooms with COVID patients, wtf? A: Dr.H: That is an Infection Prevention and Control Team decision it really is about maximizing our ability to care for people. This is only for asymptomatic people in place and there are some additional precautions. That’s a room by room and ward by ward decision. (FYI, from other sources, I heard that they won’t bunk a COVID-19 patient with someone who is unvaccinated.) Dix added: You have to remember that there are a shitton of people in hospital right now, and a shitton of people sick, and ya gotta do what ya gotta do. (<- nowhere near direct quotes)
Q: What about people who are going to need a test to prove that they had COVID-19 in order to get treatment for Long COVID? Or to travel? A: We can do antibody tests post-hoc, it’s not a prereq for getting treatment. We’re also seeing that vaccination reduced the risk of Long COVID by over 50% for Delta. Regarding travel, many countries are doing away with that requirement, and there are private companies where you can get tested, it’s just not something that the province is going to pay for.
Q: What if a LTHC runs out of RATs, will the visitors be denied access? A: We will not deny access. If they run out, than people who were negative the day before will be allowed in assuming they pass the regular symptom screening.
Q: What are your plans for allocating more RATs to LTCH? A: Dix: Between now and middle of Feb we are getting 15.7M, and they are co-top priority with hospitals, so they will get tests.
Q: Service reductions in Interior Health, mayors said they were not told about the changes, wtf? A: The plans are in place because of Omicron something something, and we done told the mayors.
Q: The message has been stay home if you’re sick, but what if you are out of sick days? A: Dix: We now have five sick days in BC which is better than other places, but yeah, it sucks. We should maybe have more days, but five is a good start.
Q: West Van wants vax clinics in schools, will you consider that? A: Absolutely, that’s been done in some places already, but that’s a school-by-school decision in conjunction with the MHO. Dix: we getting up to 50% of kids vaxxed, it varies a lot across the province; in VCH it’s more like 65%. We’ve gotten good results in community clinics for the older kids, and in the schools sometimes don’t do well.
Q: It sounds like you’re preparing people for the long haul, and that’s depressing for the clinically extremely vulnerable (CEV). A: I hope this isn’t how we live, and three doses does make a tremendous help, even for those with compromised immune systems, and we’ve been hard-asses about the six-month dose interval because there is increasing evidence that that gives longer-lasting protection for the whatever comes next. However, we are going to have to live with this, but I hope that eventually we’ll see smaller and smaller oscillations, but it is a reality that old/babies/CEVs are going to be more at risk, just like they are more at risk for e.g. influenza. I am hoping that with the immunity we have from vax and infection, that we’ll have a more gentle spring and summer, and then we’ll see what happens in the fall.
Statistics
+2,364 cases, +9 deaths, +2,526 first doses, +1,405 second doses, +53,862 other doses
Currently 924 in hospital / 130 in ICU, 33,997 active cases, 269,137 recovered.
Positivity rate of Positivity rate of 19.4%.
| first doses | second doses | third doses | |
| of adults | 92.9% | 90.3% | 40.5% |
| of over-12s | 92.5% | 89.8% | 37.8% |
| of over-5s | 89.4% | 83.5% | * |
| of all BCers | 87.0% | 81.2% | 34.4% |
Charts
From this Twitter thread:


From the federal vaccine page, first doses:

Second doses:

Third doses:
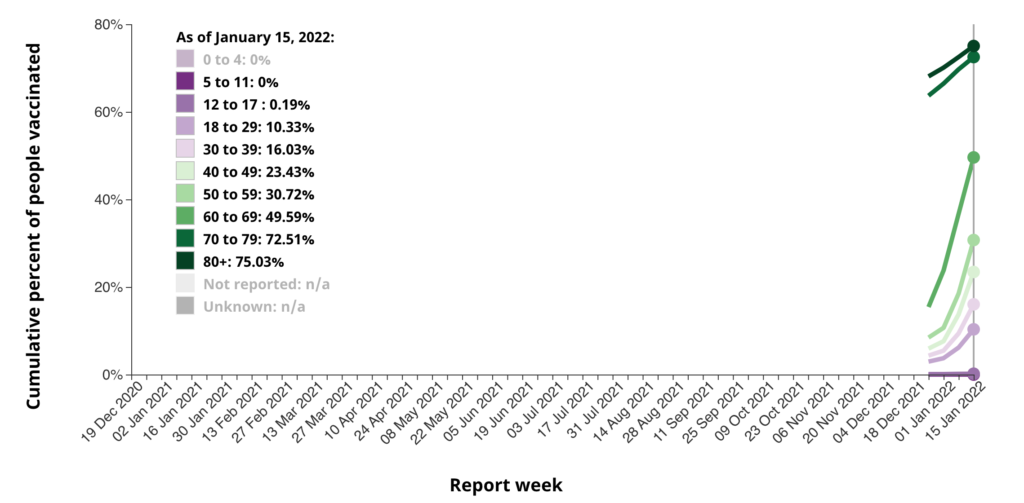
Note that these don’t seem quite consistent with the pie charts above which show the 19-29 year-olds as having the smallest slice of unvaccinated (red). I have no explanation.




