
COVID-19
Long COVID
This paper (2024-09-05) reports that baricitinib and anakinra — relatively commonly used immunomodulatory drugs — can effectively treat lung fibrosis in mice (which can cause the Long COVID symptom of shortness of breath).
This paper from USA (2024-08-26) reports that even mild COVID-19 infections can cause increased levels of autoantibodies, and Long COVID patients have even higher levels.
This paper from USA (2024-08-28) found that among people who had a COVID-19 infection diagnosis, vaccination didn’t change the risk of getting a Long COVID diagnosis.
In this article about the study, the principal investigator says she thought the earlier studies (the ones that did show that vaccination dropped the risk) were flawed because they relied on patient surveys, with the implication that electronic records would be more accurate. I think they would be less accurate! Long COVID is hugely, woefully under-diagnosed. There are still a fair number of doctors who believe that Long COVID doesn’t exist! 🙁 There are also a lot of people who never got a formal diagnosis of a COVID-19 infection (like because they couldn’t get a test or had an asymptomatic case). Addendum: A reader asked for a citation that you could get Long COVID with an asymptomatic case. You absolutely can. Your risk of Long COVID is higher the more severe your acute COVID case was, but it does not drop to zero.
In the article discussing the case, a different scientist pointed out a possible confounding cofactor: the type of patient who seeks out a long-COVID diagnosis likely uses healthcare and is vaccinated.
By the way, even this study found that 6.9% of people diagnosed with COVID-19 get Long COVID.
This paper from Italy (2024-09-05) found that Long COVID in kids mostly dropped over time, with the percentage at various follow-up points being:
- 23.2% at 3 months;
- 13.2% at 6 months;
- 7.9% at 12 months;
- 6.1% at 18 months;
- 7.1% at 24 months.
The most common symptoms were fatigue (13.1%), shortness of breath (6.3%), headache (5.9%), and gastrointestinal symptoms (4.9%).
The authors were sloppy about specifying what the control group was, but I think it is just the opposite of what they specify, so “female” would be compared to “male”. Given that uncertainty, they described a lot of increased risks at three months:
- over 12 years old, 11.33 time higher risk;
- comorbidities, 1.83x;
- being infected with original variants, 4.77x;
- being female, 1.62x;
Some stayed risk factors for at least 18 months:
- over 12 y/o, 9.37x;
- infection with COVID Classic, 3.52x,
- infection with Alpha, 4.09x.
Warning: I found the paper a bit difficult to slog through: they tended not to give details which I kind of wanted (like what their comparison groups were!), and I couldn’t understand the labels on their graphs.
This paper from USA (2024-08-19) reports that ME/CFS patients with orthostatic imbalance (i.e. have a crash in blood pressure when they stand up) have elevated levels of tetrahydrobiopterin, which is used in the production of nitric oxide, which widens blood vessels. More tetrahydrobiopterin leads to wider blood vessels, which leads lower blood pressure. (🎶 Hello darkness my old friend 🎶, I stood up too fast again! 🎶)
This paper from USA (2024-07-31) reports that, based on electronic records, Paxlovid didn’t help reduce new-onset cognitive, fatigue, and respiratory symptoms after a COVID-19 infection.
COVID-Related Excess Deaths and Sickness
This paper from Romania (2024-08-28) reports that 75% of patients who developed Long COVID after hospitalization for COVID went on to develop diabetes within a year.
Mental Health
This paper from Japan (2024-08-21) reports that playing video games improved mental health and life satisfaction during the first two years of the pandemic.
Vaccines
This article (2024-09-06) reports (halfway down, keep scrolling!) that Canada will be getting ~19 million doses of mRNA vaccines (assuming they get approved, which they will). That is only enough to vaccinate a bit less than HALF of all Canadians! Even if you only vaccinate adults, there’s still only enough vax to vaccinate ~55% of the adults.
The article also says Health Canada is reviewing Novavax, but “Canada’s current contract with Novavax only provides access to domestically manufactured vaccines, which Novavax has been unable to confirm for the 2024/25 season”.
Huh?? Moderna opened a plant in Laval (2024-02-23), but I couldn’t find anything about Pfizer manufacturing in Canada!
The only site that Pfizer lists in Canada is in Brandon MB, but their corporate site says that they make “conjugated estrogens” in Brandon. This Pfizer/BNT press release (2024-05-08) says “Pfizer and BioNTech have provided an expression of interest for possible supply to the COVAX Facility”, but nothing about them actually moving in.
Anyway. The article about deliveries goes on to say that if Health Canada doesn’t approve Novavax, then provinces are free to buy it themselves, but there’s not enough demand at a province level to make it worthwhile to buy. (Only 5,529 doses of Novavax were administered by 2024-06-31.) It looks like you’ll need to go to the USA and pay for it if you really want Novavax. 🙁
This article from USA (2024-09-04) points out that if you have “a cold” (which IMHO is probably COVID-19!) there is a good reason to find out if it is COVID-19 or not, even if the knowledge doesn’t change your immediate behaviour: because it could influence when you get your next shot. If you only get a limited number of shots like in Canada, you should wait until about four months since your infection to get your next vaccine. (It probably won’t hurt you to get another shot, it just might not be as effective.)
This article (2024-09-04) reports that some people in the know don’t think that the fall COVID-19 vaccines are going to be ready to go into arms in Canada until October.
This might only be interesting to me, but this paper from USA (2024-08-20) says that infections mostly give antibodies to the nucleocapsid and the spike’s N-Terminal Domain, while the vaccines mostly give antibodies to the spike’s Receptor Binding Domain.
There have been a lot of really promising studies of vaccines in animals recently. Those papers aren’t going to turn into vaccines that you can get for several years, so you might want to skip down to Pathology below if you only care about immediate things.
***
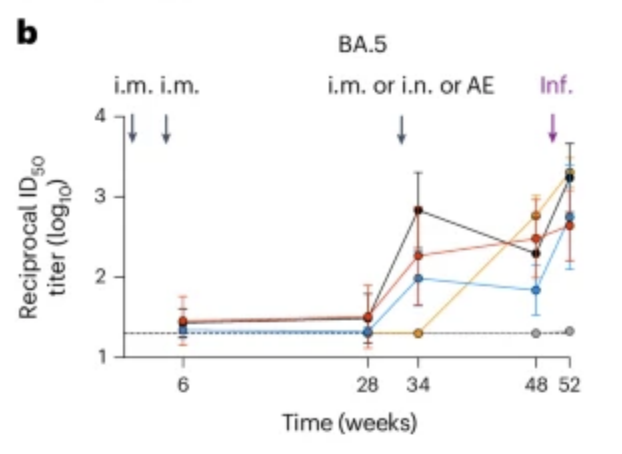
This paper (2024-09-03) reports that a mucousal vaccination of monkeys really kills viruses in their noses.
In the graph below, the y axis is the amount of culturable virus on nasal swabs (top) and in nasal rinses (bottom); the x axis is days since the monkeys were deliberately infected with XBB.1.6. red, blue, and orange are are mucousal administration and the others are intramuscular injections (but orange is only one dose of anything);
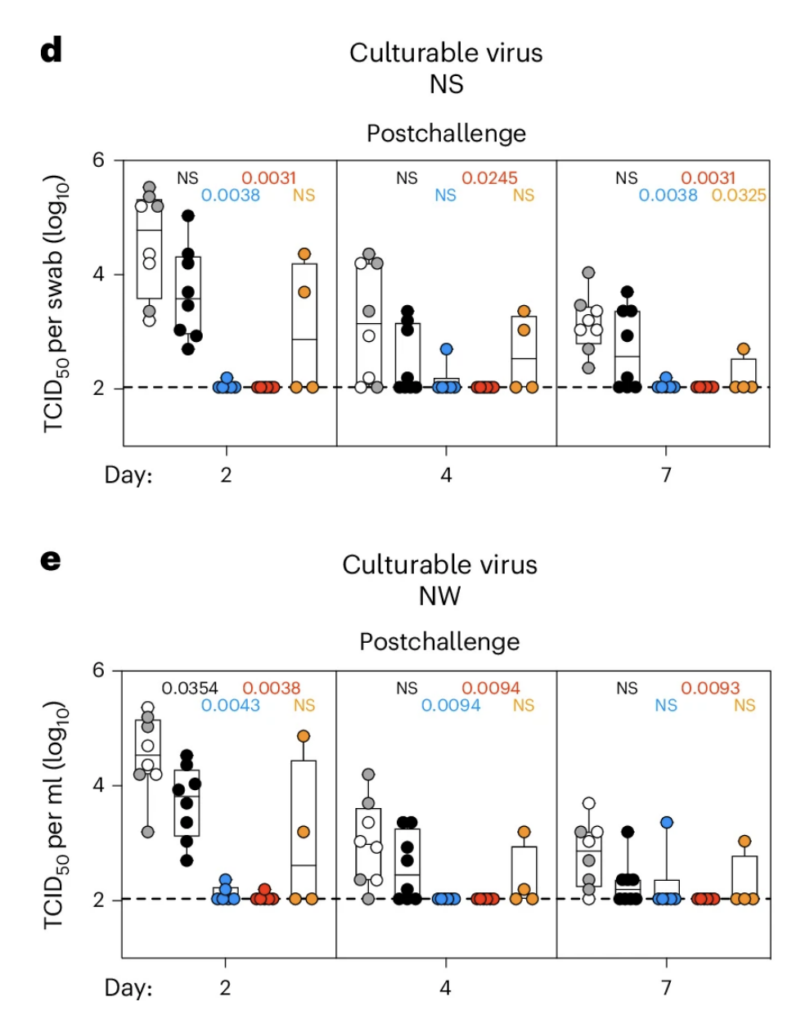
grey: 2 mRNA injections + 1 viral vector injection
black: 2 Moderna Classic injections + 1 Moderna Classic/BA.5 bivalent
blue: 2 Moderna Classic + 1 intranasal BA.5-based viral vector
red: 2 Moderna Classic + 1 inhaled BA.5-based viral vector
orange: 1 inhaled BA.5-based viral vector
The authors tried to say that the mucousals were durable, but honestly they didn’t look any more durable than two Moderna Classic plus Moderna Classic/BA.5 bivalent (which surprised me at how good it looked, even after 52 weeks):
***
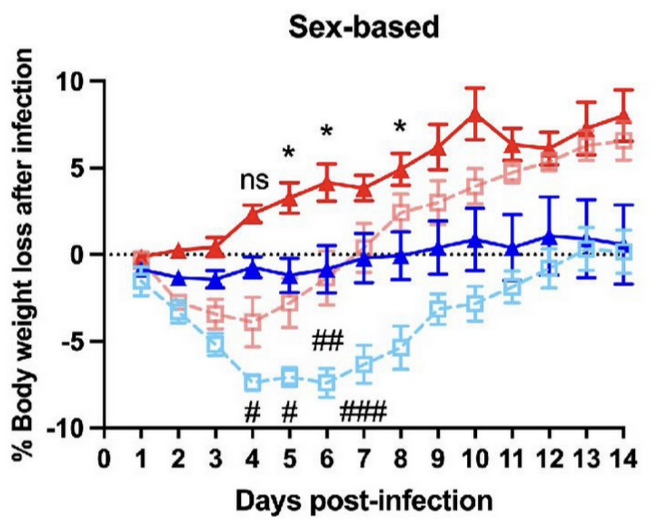
This paper (2024-08-29) reports on tests in rodents of an intranasal adenoviral vector-based COVID-19 vaccine, which isn’t that novel or interesting except that they broke out some results by sex of the rodent. Look how much better the female rodents did than the male rodents!
This graph shows the results of administering one dose of the vax, then deliberately infecting the rodent three weeks later. The y-axis is the weight gain, which is widely used as a proxy for “how sick do they get”. Red is vaxxed female rodents, blue is vaxxed male rodents, pink is unvaxxed female rodents, baby blue is unvaxxed male rodents:
***
This paper (2024-08-27) reports yet more promising results in rodents, this time using an intramuscular vax which takes an Omicron spike with the 6-proline stabilization (HexaPro), but with a MERS Receptor Binding Domain (RBD) instead of the Omicron one. Mice that were given a BA.5 shot and then a booster with the Franken-MERS shot had good protection from SARS-CoV-1, SARS-CoV-2, and MERS!
***
This paper (2024-08-26) reports that chimeric spikes give good protection to mice. They made mRNA for a bunch of different Frankenspike types with the RBD from one virus, the N-terminal domain from another virus, and the S2 (based) part of the spike from another. They mixed&matched with pieces from SARS-CoV-1, SARS-CoV-2, HKU3-1 (a bat virus), and RsSHC014 (a bat virus). They then gave mice different cocktails of 1 to 4 of the different Frankenspikes (plus some controls).
Most of the cocktails gave the mice protection in test tubes against a subset of different coronaviruses (including a pangolin coronavirus!), but none gave protection against all of them. (Most didn’t help against the “common cold” coronaviruses, alas.) Mice that were given the cocktail with the highest number (four) of different Frankenspikes did not get sick when challenged by SARS-CoV-1, SARS-CoV-2 Beta, or WIV-1 (yet another bat coronavirus).
Pathology
This paper from USA (2024-09-04) reports that pregnant women had higher risks of gestational diabetes, hypertensive disorders, and gestational weight gain early in the COVID-19 pandemic.
Transmission
This release from the US CDC (2024-08-23) says that US hospitals will be required to report flu, COVID-19 and RSV cases again, starting on 1 November 2024. It’s not Canada, but the US is nearby, so this improved data reporting is still of some value to us.
This ambitious paper from France (2024-09-04) tried to figure out how dangerous various activities were. They surveyed people who had just gotten COVID-19 about where they had been in the previous week, and split them into groups based on what mitigation measures were in force when they caught COVID-19. They then compared them to controls who they also surveyed.
The results were… kind of all over the place.
They used “worked in a location without open space” as their reference, which I found slightly odd because lots of people were working from home — at least in Canada — in October 2020, which is when the paper started. (NB: There’s no information in the paper about whether people masked at work or not, or what “open space” here means. Does a grocery store have “open space”, or are they only talking about “open plan offices”?)
But also, some of the things didn’t make much sense to me. Compared to going-to-work-without-an-open-space:
- going to a concert was 15% lower risk during a period where the only mitigations required were a mask in public spaces, but going to a concert was twice as risky as going-to-work-without-an-open-space in the period where you had to mask AND you had to have proof of vaccination;
- going to a nightclub was more than twice as dangerous in the first two periods where you could go to a nightclub (and the risk dropped from there) but going to a bar during the same period started out being only 28% higher risk, and dropped to about-the-same risk for two periods, and ended up being about 10% less risky;
- going to a restaurant was always about 10% less risky (!);
- going to work in a location with open space was 10% to 57% more risky;
- going to a party was significantly riskier at any point, but going to a private party was less risky.
Also: presumably people spent ~8 hrs per day at work, while going to the supermarket or a restaurant presumably took much less time.
Bottom line: I don’t know how to interpret this study.
Recommended Reading
Hilda Bastian is my go-to for vaccine news. I’ve incorporated some of her most recent post (2024-08-31) into this post, but not all of it.
This article from USA (2024-09-03) discusses how prepandemic Italy and Texas emphasized hospitals over primary care, what they were doing about the weaknesses that emphasis revealed, and what the new Italian clinics look like. It only touches lightly on the pandemic, but it’s an interesting look at primary-focused care.
This blog post (2024-09-03) is suuuuper long and suuuuper detailed/technical about the strengths and weaknesses of the Novavax vaccines. Tl;dr: he doesn’t like Novavax as much as I do (well, did, before reading his post).
Mpox
Transmission
Mpox is airborne, y’all! This older article from Belgium (2023-07-24) and this one from Spain (2023-03-24) reports that they were able to detect mpox in the air at a clinic and at nightclubs.
Some good news! This US CDC report (2024-09-05) found that in relatively extensive contact tracing of clade 2 mpox cases on US flights, there were zero cases of other people catching clade 2 mpox on those flights. (Clade 2 was the one spreading two years ago, and is less lethal than the Clade 1 which has got people scared right now.)
Vaccines
This paper from Moderna (2024-09-04) reports that their mRNA vaccine protected monkeys from an mpox infection better than Bavarian Nordic’s Jynneos vaccine did. All of the monkeys survived being deliberately infected, but the Moderna-vaccinated monkeys had significantly fewer lesions (which is a good proxy for disease severity) than the Jynneos monkeys did. The Jynneos-vaccinated monkeys’ lesions also took ten days longer to disappear than the Moderna-vaccinated monkeys’ did.
It’s buried in the paper, but more obvious in this article (2024-09-04) about the study: Moderna’s vax presents four proteins which are found in all poxes, so it is likely that the Moderna vax will also immunize against smallpox, cowpox, horsepox, etc. (Chicken pox is from a different family, sorry, but it’s got its own vax.)
HPAI (Bird flu)
Transmission
This press release (2024-09-06) reports that a human with no obvious animal exposure tested positive for H5N1. The good news is that they found it with routine flu surveillance.
This article (2024-08-30) reports that three California cow herds have tested positive for highly pathogenic avian influenza.