
Vaccines
People ask me which vaccine they should get. I tell them it’s really between the Pfizer BA.4/5 bivalent and the Novavax, that I don’t have enough information to distinguish between those two. This paper from Novavax with data from South Africa says that three doses of Novavax works about as well as — not really better or worse — than three doses of mRNA. I think that means the monovalent mRNA, but I can’t tell.
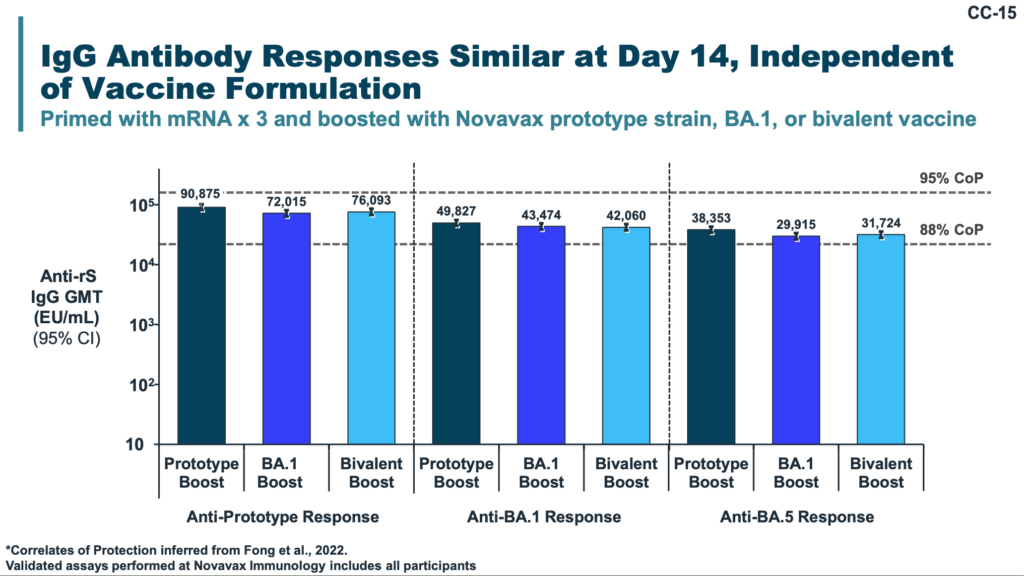
This presentation today from today’s presentation to the US CDC says, among other things, that blood from Novavax vacinees with COVID Classic, monovalent BA.1, and bivalent Classic/BA.1 all had really similar antibody levels. This was true regardless of whether they were looking at Classic, BA.1, and BA.5. In other words, the fact that it’s not a bivalent booster doesn’t matter much.
Novavax has a macho adjuvant, and I have seen a theory that adjuvants somehow (me waves hands) help give broader protection, and that this data does suggest that Novavax gives broader protection.
So…. I still don’t know what to recommend. I suspect that Pfizer’s bivalent is better at what is circulating right now, but that Novavax is probably going to be better at whatever strain comes later.
Now, the Pfizer bivalent BA.4/5 is much easier to get in BC than Novavax. It’s what all the pharmacies are going to have as a default value. (You might be able to get the Moderna bivalent if you try, but I wouldn’t. I believe that the Moderna which Canada bought is bivalent with BA.1, which is not as effective.)
This report from the USA looks at how good the bivalent mRNA boosters’ vaccine effectiveness (compared to people who did not get a booster) is against symptomatic infection for BA.5 and XBB.1.5:
| Age | BA.5 VE | XBB.1.5 VE |
| 18–49 years | 52% | 49% |
| 50–64 years | 43% | 40% |
| ≥65 years | 37% | 43% |
That’s actually pretty good!
While the side effects of vaccination are normally both rarer and milder than the effects of COVID, vaccine injury does happen. This preprint from New Zealand found that, in addition to the occasional myo/pericarditis (a 2.6x risk after the first dose and 3.1x risk after the second dose compared to unvaccinated), they also saw higher risk of acute kidney injury: 1.6x after first doses and 1.7x after second doses.
Just because I feel like I have to keep telling people that the bivalent vaccines are better, this preprint from Sweden / Norway / Finland / Denmark says that the bivalent mRNA vax as a fourth dose is ~80% more effective against hospitalization than three mRNA doses without a booster. BA.4/5 on the left, BA.1 on the right:

This correspondence from the USA showed very similar Vaccine Effectiveness results of one or two mRNA boosters (compared to no boosters):
| against | # boosters | monovalent VE | bivalent VE |
| hospitalization, days 15-99 | 1 | 15.8% | 54.0% |
| hospitalization or death, days 15-99 | 1 | 4.2% | 54.0% |
| hospitalization, days 15-99 | 2 | 28.0% | 61.9% |
| hospitalization or death, days 15-99 | 2 | 32.2% | 64.0% |
| hospitalization, days 15-99 | 3 | N/A | 55.7% |
| hospitalization or death, days 15-99 | 3 | N/A | 63.1% |
The bivalent booster’s effectiveness also did not wane as fast:

This press release reports that India has approved Bharat Biotech’s iNCOVACC, a nasal vaccine. Effectiveness data has not been published yet.
Long COVID
Good news! This case study (one patient) and this case study (two patients) say that a stellate ganglion block — an injection of anesthetic into nerves which run alongside your voicebox in the neck — can restore lost sense of smell. This anecdata says that a clinic in Texas is having great success with stellate ganglion blocks.
This case study (one patient) says that a stellate ganglion block helped a patient with fatigue, post-exertional malaise, shortness of breath, and gastrointestinal symptoms. Maybe stellate ganglion blocks can help all kinds of Long COVID!
This preprint found that people who took a long time (more than 28 days to test negative on a PCR test after their first positive test) were 54% more likely to have brain fog and 72% more likely to have muscle pain that people who cleared in less than 28 days.

Among other things, this paper from Germany found that, while 53% of patients felt they had improved, only 9% of Long COVID patients felt they had made a full recovery 22 months after their initial sickness.

Only 40% had returned to full-time work:

This article reports on this report from New York State’s largest workers compensation fund found that about 18% of their Long COVID claimants have been unable to return to work for a year or more; three-fourths of those were under 60. (Note that this covers only people entitled to workers’ compensation, i.e. those who could reasonably prove that they caught it at work, and those capable/determined enough to file a claim.)
This report from the USA found that students/faculty/staff at a university who had just a primary series were slightly more likely to get Long COVID (as defined by symptoms for more than 28 days), but people who had a booster were way less likely:
- No vax: 47.7% chance of Long COVID
- Primary only: 44.4% chance of Long COVID
- Booster: 25.9% chance of Long COVID
This is worrying. This preprint from France found that the risks in children of acute tubulointerstitial nephritis (kidney infection) was higher after a COVID-19 infection. The absolute numbers were low — only 41 kids in all of France — but the relative risk was very high. The risk of acute tubulointerstitial nephritis without uveitis was 3x higher and the risk of acute tubulointerstitial nephritis with uveitis was 12x higher. This is just more proof that COVID-19 f’s with the whole body.
This paper from Taiwan says that getting a COVID-19 infection gives a higher risk of a long list of auto-immune disorders. Over two years, the risk of getting these things for people who had a COVID-19 infection vs. those who had not gotten infected was:
- rheumatoid arthritis: 2.98x;
- ankylosing spondylitis: 3.21x;
- systemic lupus erythematosus:2.99x;
- dermatopolymyositis:1.96x;
- systemic sclerosis: 2.58x;
- Sjögren’s syndrome: 2.62x;
- mixed connective tissue disease: 3.14x;
- Behçet’s disease: 2.32x;
- polymyalgia rheumatica: 2.90x;
- vasculitis: 1.96x;
- psoriasis: 2.91x;
- inflammatory bowel disease: 1.78x;
- celiac disease: 2.68x;
- type 1 diabetes mellitus: 2.68x.
This is all on top of a 1.2x risk of death.
The American Heart Association found that cardiovascular deaths went up by a lot (6%, which is a lot) during the first year of the pandemic.
Pathology
This paper from Australia says that kids’ innate immune system is better at adults at killing off novel pathogens like COVID-19. However, there’s a cost: because they kill it off so fast, their adaptive immune system doesn’t get as good a look at it, so doesn’t help them avoid reinfection as much.
Mitigation Measures
This article says CRA would like to remind you that COVID-19 mitigation payments are taxable, and need to be reported.
Misinformation
This article says that misinformation cost Canada 2,800 lives and $300M over (just) a nine month pandemic period.
Recommended Reading
This article from the USA does not apply completely, but it talks positively about treating patients in their homes instead of in hospital.
This article from California says that the percentage of people dying at home is increasing, and explores reasons why. (Spoiler: hospitals are not fun places.)