Press Briefing
Here is what I found interesting/novel in today’s briefing (video, slides):
Paxlovid
- BC has 4000 doses coming (or here already? unclear), and that’s way fewer than the number of cases.
- Paxlovid has to be started within five days of symptoms. DrH said they have set up a “hub and spoke” model so that the drugs can get to the patients very quickly.
- DrH said that the BC COVID-19 Therapeutics Committee looked at it and decided to give it to clinically extremely vulnerably people (CEV) Groups 1 and 2. (I don’t know what those are, but I would guess that Group 1 would be e.g. immunocompromised or on dialysis, while Group 2 would be e.g. diabetics.) I was slightly surprised that “elderly” were not at the top of the list, but then realized that boosters still work on the elderly, AND many (most?) elderly also have conditions that would put them on a CEV list. Note that “unvaccinated” was not given as a criterion.
- The two drugs in Paxlovid have a shitton of drug interactions, frequently with the exact drugs (especially immunosuppressants and anti-coagulants) that the CEVs are on. ☹️ DrH said that they are going to proactively contact the CEVs and remind them to keep getting tested (which I think means COVID testing) and to let them know if they qualify for Paxlovid.
- Paxlovid is very new, so they are still learning about side effects and drug interactions.
Hospitalizations
The slides were mostly about hospitalization with COVID-19 vs. because of COVID-19, and how Delta and Omicron differed.
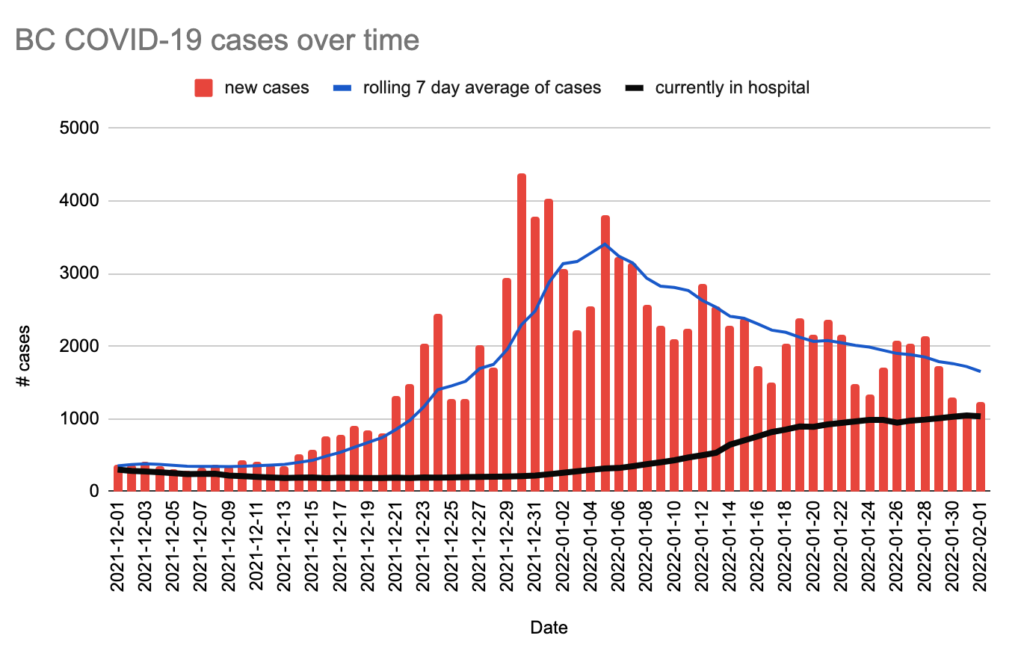
Hospitalizations are a lagging indicator, but they are starting to go down. Yes, we have a record number of people in hospital, but the number entering per day is going down:

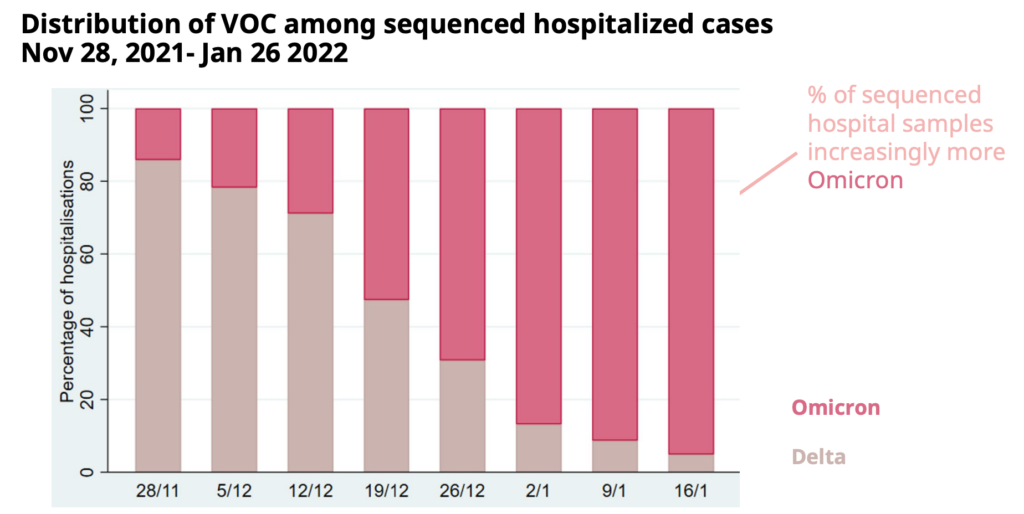
The cases are becoming more and more Omicron, but there are still a number of Delta cases hanging on:
Delta and Omicron have quite distinct characteristics:

DrH called out that for Omicron, the percentage of vaccinated people being admitted is much higher than for Delta. She said that was because a good portion of the Omicron people were admitted for non-COVID things. At the beginning of Omicron, the median age was lower for Omicron than Delta, and so they weren’t sure if Omicron actually was milder or just looked milder because the infected were younger. Now they can tell that Omicron really is milder.
The proportion of patients over 80 is higher, which says that being old is a risk factor. Also remember that the very old have more comorbidities. And maybe the over-80s had not gotten boosters yet during Delta?
The length of stay for Omicron is about half that for Delta. A lot of the people who were admitted in December or January are still there (? I thought the median stay was 3 or 7 days?), and a lot of those are still Delta.
There are also far fewer people needing critical care for Omicron than Delta — only 35% as many. The death rate is also less than half.
They did a detailed look at 550 charts from Dec.1 onwards, province-wide, to see if they were there for COVID-19 or with COVID-19, and found that about 44% were with and not for; 40% needed hospitalization but not ICU, and 16% needed ICU.
Broken down by variant, there are a lot more with cases for Omicron than Delta. (The unknowns are too recent for the sequencing to be done, so they are going to be mostly Omicron.)
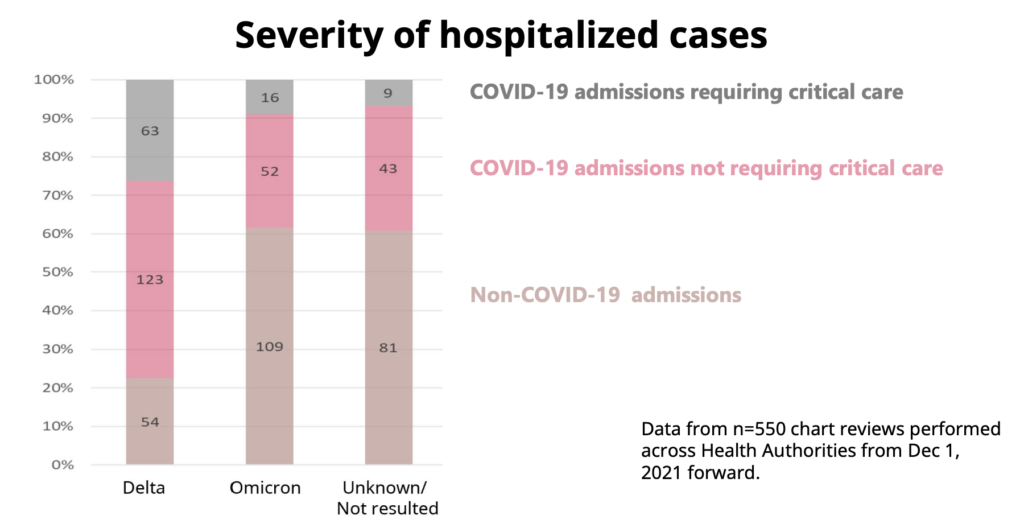
Broken out by vax status:

I thought it was interesting that Omicron vaxxed is about 65% with and Unknown — i.e. recent — is 75% with. I bet that is because the more recent admits are more likely to have been boosted.
They broke it down by age also:
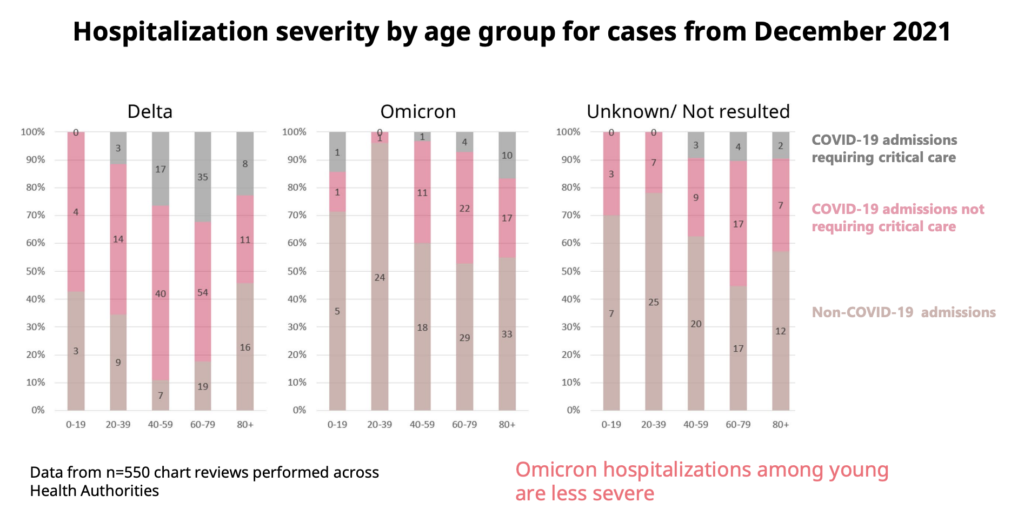
This shows that Omicron cases in the young are much less severe than Delta cases.
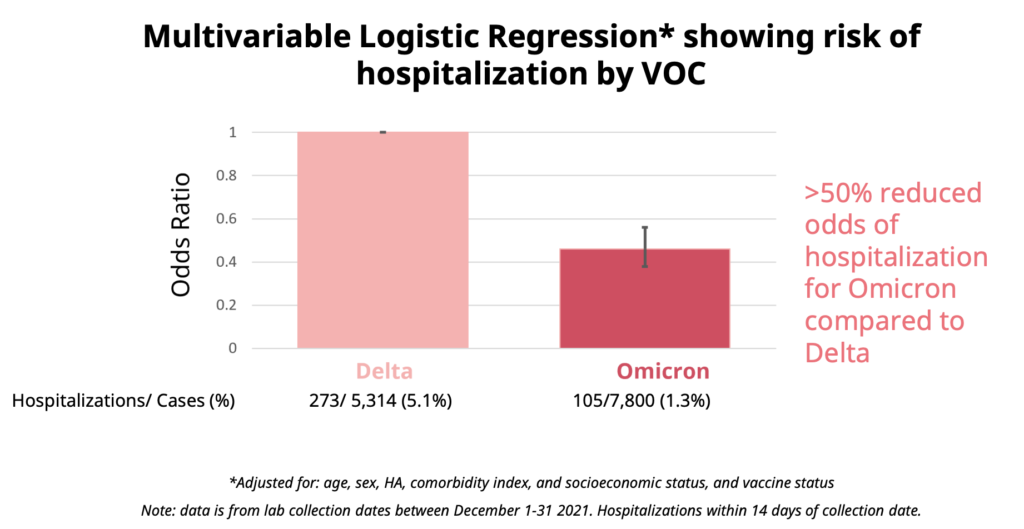
Adjusted for age, vax status, health authority, comorbidities, and socioeconomic index, you’re about half as likely to be hospitalized for Omicron as for Delta:
Long-Term Care Homes
DrH said that earlier in the pandemic, we had to have very strict, one-size-fits-all outbreak measures because it was SO scary. (<- “Scary” is my word, not hers.) Now that things have calmed down, we have vax, we have milder variant, we don’t need the ultra-strict one-size-fits-all, we can have more nuanced measures. New guidelines will go up on the BC CDC website today for management of LTCH and visitors. DrH reminded everyone that the December Measures for visitors — including that they have to be vaxxed, wear PPE at all times, and only visit their person.
DrH talked quite a bit about how there has “always” been one essential visitor allowed, and those are people who help with care. About a third of LTCH residents have an essential visitor. LTCH residents are also allowed one “designated visitor” (which has also sometimes been called a “social visitor”). I was a bit confused if the designated visitor was new or not. It also seemed at one point that the essential visitor would still be allowed in, even during outbreaks, while the designated visitor would not. Later, it seemed that the designated visitor would also be allowed in during outbreaks. I was confused.
DrH said that calling an outbreak was a judgement call determined by the MHO, Infection Control Teams, and the facility. The guidance for how to communicate has changed a bit and will be up on the web site. I was a little confused here, and so, it turns out, were reporters.
DrH alluded to maybe lifting some restrictions in mid-February.
Vaccinations
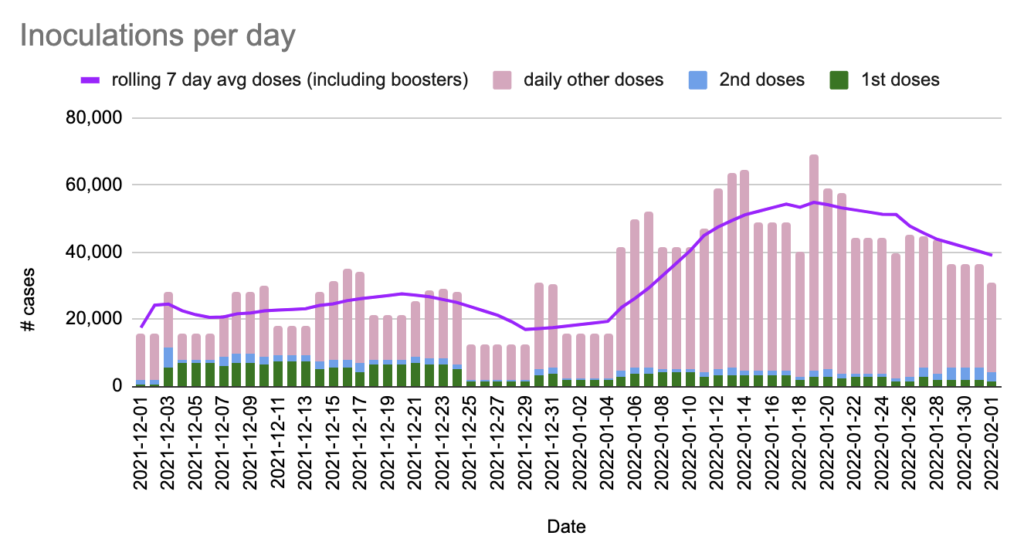
Dix rolled off numbers, and mentioned that the half of the five-to-eleven year-olds have now gotten at least one shot.
Acute Care
BC hospitals have 9229 base beds, of which 8776 are full. There are 2353 surge beds, of which 582 are full.
For ICU beds, there are 510 base ICU beds, of which 448 are full. There are 218 surge ICU beds, of which 30 are full.
So there are more patients than base beds, but not as many patients as surge+base. The system is straining but not overwhelmed.
From Jan 24 to Jan 30, 17K HCW called in sick (9%). (That’s people, not days, not shifts.) This is almost identical to the past two weeks. So while it’s not getting better, it’s not getting worse, either.
He gave the breakdown of sick HCWs by Health Authority. You can go look it up in the video if you care, at about 31:38.
Rapid Antigen Tests
Dix gave numbers for RATs. ~2.7M arrived in the past three days. A bunch are getting delivered various places (look it up, about 33:49). BC is now expecting 16.6M tests between now and the middle of February. This is a change from 15.7M that they were expecting last week.
Surgical Renewal (i.e. postponed scheduled surgeries)
Dix gave numbers for that, and I’m sorry, I don’t care any more. I have the impression that they aren’t cancelling ALL surgeries like they did before. You can look up the numbers at about 35:08.
Pediatric Boosters
DrH mentioned that NACI came out with a recommendation for a 6-month interval for boosters for 12-17 year olds, which is what BC is using. Also, they advised an extra dose for CEV teens, which BC was going to do. Carry on.
Q&A
Reminder: I summarize and snarkify heavily.
Q: Um, what is going on with changing the guidance for LTCH? Did you already make that change in December and not tell us about it? A: Look, the guidance has always been guidance that the MHO and Infection Control Team and facility would interpret on a case-by-case basis. That guidance is kind of out of date because Omicron is so much less destructive, so the MHOs and Infection Control Team were ignoring it more and more, so we updated the written guidance. (<- That is VERY VERY heavily my reading between the lines.)
Q: Um, what does it mean now to declare an outbreak? A: If there is spread and we don’t know where it is coming from. If there’s a staff member who’s got it, but they are at home, that’s not an outbreak. If there’s one resident who clearly caught it from the community, and they are now isolating in their room, that’s not an outbreak.
Q: You’ve got 3M rapid antigen tests, why can’t you get those out to people who want them, so they don’t have to call around to pharmacies to try to find some. Release the RATs!!! A: First, a lot of those 3M are in transit: they came in within the past three days and are getting sent out again pretty much right away. Second, do you even know how to do long division? Do you realize that 3M is less than one per person? We can’t give everybody unlimited RATs, so we are prioritizing to where we think they will do the most good. When supply is no longer an issue, then we’ll work to get them out to randos. (<- WAAAAAY snarkified because I am getting really tired of this question. I would go nuts having to answer the same question over and over and over and over.)
Q: Uh, wtf designated and essential visitors? A: Essential visitors help with care. Designated visitors are social. Both are chosen by the resident, and every resident is entitled to two. They can come regardless of outbreak status.
Q: There was a specific case of a woman who the hospital called and said she’d have to feed her 87 year-old mother because the hospital was short staffed, wtf? A: As we’ve told you again and again, we can’t comment on specific cases. There are times when family helps, either because they want to or the patient asked for it or the hospital thinks it would be beneficial. (I can imagine if the patient is confused or hostile, it might help to have a familiar face.) But chill, Mom isn’t going to starve, someone will feed her. If you have a complaint, follow the complaint process.
Q: Pfizer is working at getting its under-five vax approved, when do you think we’ll get that vax in BC? A: Pfizer is working with the US FDA on that, the US is a completely different country with a different process. The FDA asked them to give the interim two-dose results so they could work on it while they wait for the third dose results. Pfizer has not yet given Canada the data package.
Q: NB: I didn’t understand the question. It was not well-phrased. I’m going to guess at what the reporter meant, but I am really not sure. People are wanting to go on Spring Break, but you can test positive on a PCR test for a while after you’ve actually recovered. There are provisions for not needing to test again if you can show that you had COVID-19, but that’s now not available for lots of people. Is there a way that the province can provide documentation for people who tested positive with a RAT? A: This is not a BC-only problem. And the publically-funded PCR tests are not for private personal travel. There are some private clinics which can verify RATs at the person’s own expense. But really, it’s unlikely that if you have COVID-19 now, you’ll still be positive in March when Spring Break rolls around.
Q: Have you had any discussions with your federal counterparts about simplifying the confusing testing requirements for travel? A: Yes.
Q: It seems like the public, visitors, and residents ought to know if COVID-19 is spreading in the facility. Why don’t you still declare outbreaks publicly and then choose how to respond (instead of not declaring an outbreak)? A: Because it’s not dangerous, the public doesn’t need to know. Ducky’s answer would have been, “because if we declared an outbreak every time one resident or one staff got sick, every single LTCH would be on outbreak, and so the term “outbreak” would be meaningless.” Residents and their families are notified if someone at the facility has COVID-19.
Q: Really, why don’t you declare outbreaks so that people know when COVID-19 is circulating???? A: Look, this is how we have always done it with influenza and RSV etc. We don’t need to tell the world that there is one resident isolating with COVID-19 in a 300-bed facility.
Q: Are you going to lift all the Measures by 15 Feb? A: Not bloody likely. We’re probably going to have a lot of Measures for a lot longer — the simpler ones like mask-wearing. But I expect we’ll gradually turn up the dial to make parties possible again.
Q: Half the children have been vaccinated, and there are also kids who have had Omicron. Given that, when do you think schools will get back to normal, y’know, no masks, field trips, no distancing? A: With new variants popping up all the time, who the f knows? But hopefully, hopefully, spring and summer will look better. We’ll probably have another variant slam us in the fall, but predicting the future is hard.
Q: You said 60% of COVID-positive patients in hospital are there with and not for: how much of that is due to hospital-acquired infections from roommates? A: We have had cases in hospital where someone we did not know someone was positive who transmitted it to someone else, but I don’t know of any cases where there was someone who we knew was positive transmitted it to someone else.
Statistics
Today: +1,236 new cases, +9 deaths, +1,243 first doses, +2,742 second doses, +26,728 other doses.
Currently 1035 in hospital / 139 in ICU, 28,302 active cases, 293,488 recovered.
| first doses | second doses | third doses | |
| of adults | 93.1% | 90.5% | 49.7% |
| of over-12s | 92.7% | 90.1% | 46.4% |
| of over-5s | 89.9% | 84.0% | * |
| of all BCers | 87.5% | 81.7% | 42.2% |
Charts
From this tweet: