Treatments
This article says that it’s not just Americans being stupid: some feed stores in BC are seeing a run on ivermectin (a dewormer which the fringe right has decided is a good treatment for COVID-19, all scientific evidence to the contrary).
Press Briefing
Most of the time spent at the briefing was going over slides, most of which are also in the Biweekly Data Summary.
Where is spread happening?
Multiple times, DrH said basically that most of the province was in pretty good shape, it was just isolated pockets, mostly in the Interior and Northern HAs. I didn’t entirely believe her, but this map does make it look like that. For example, case counts are really low in the Lower Mainland and the southern Island; the case counts are up Fraser Health, VCH, and Island Health, but look at where they are happening: in VCH it’s only Bella Coola, right downtown, and DTES. In Fraser, it’s only Hope. On the Island, it’s only Port Alberni.


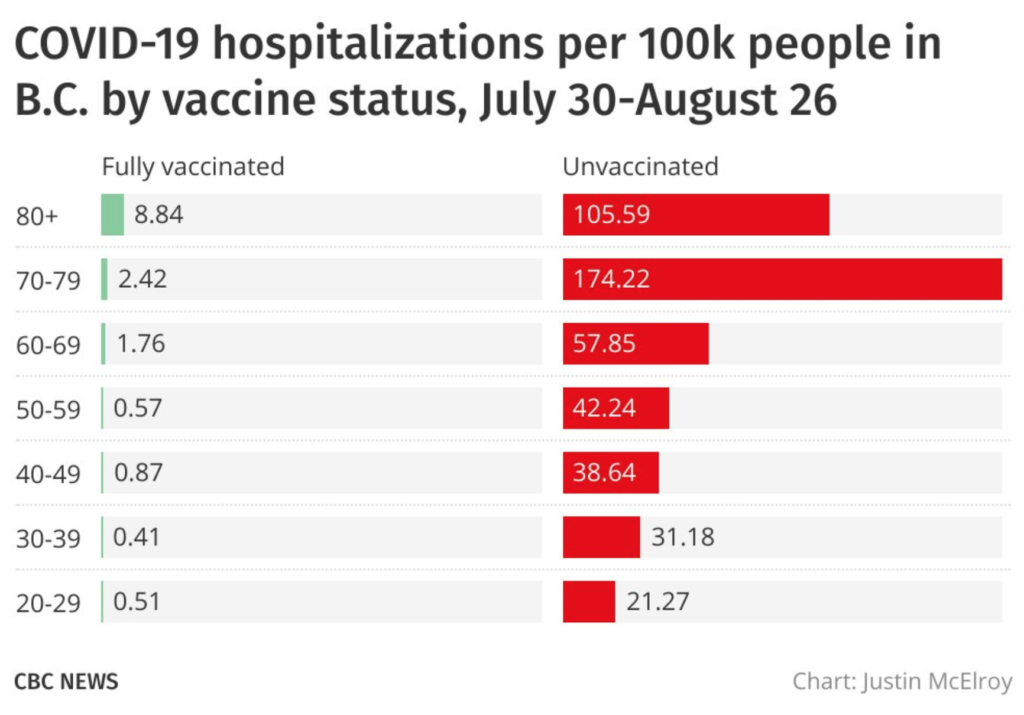
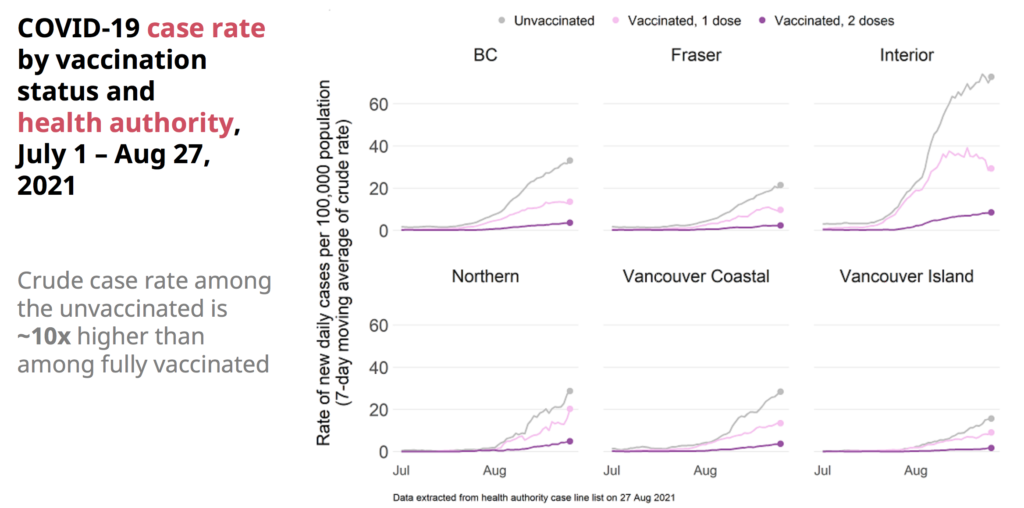
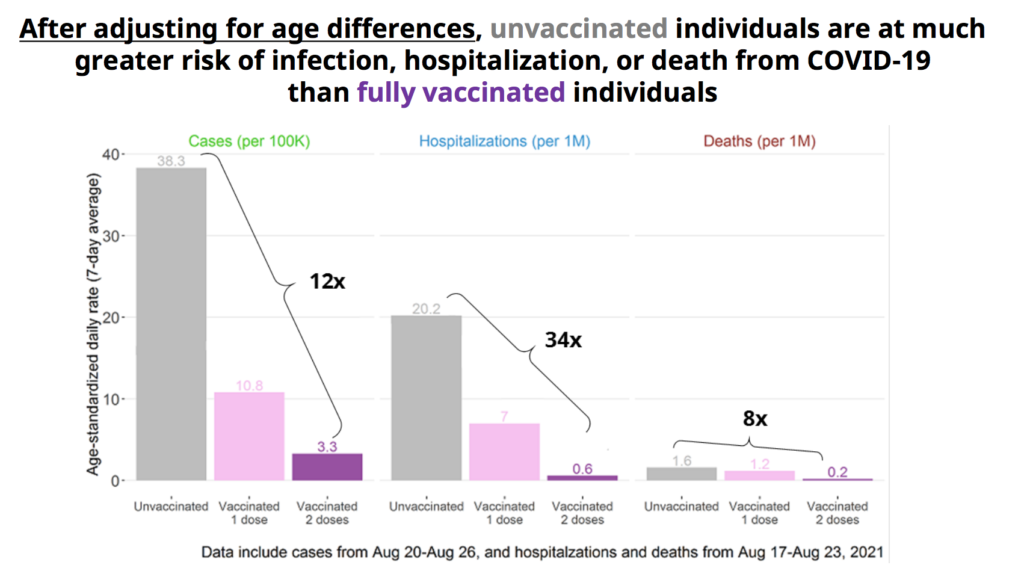
How good is vaccination?
They showed a number of graphs which showed how different the pandemic is for vaccinated vs. unvaccinated people. The differences are stark:



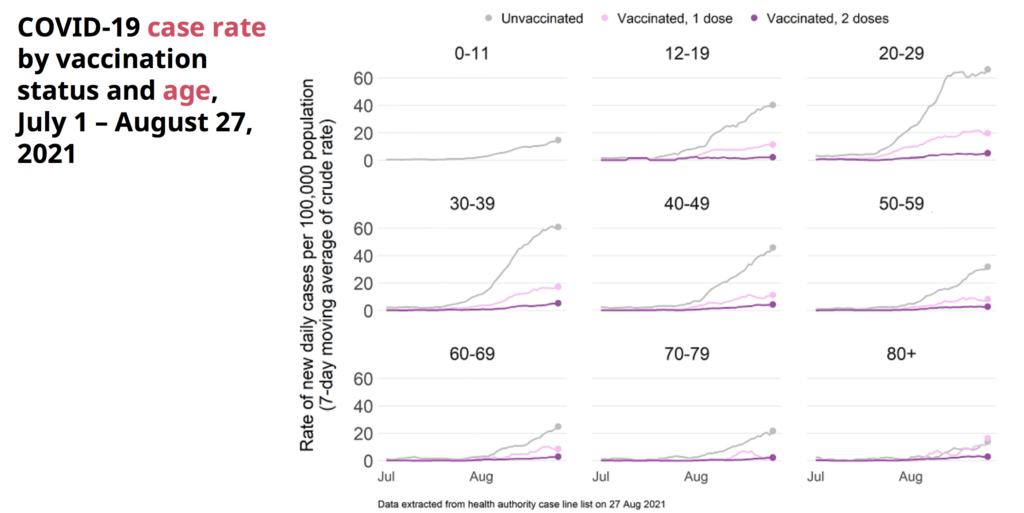


Who is getting sick?
Case counts are highest in the 20-40 year-olds:


They emphasized that they are not seeing kids get hit harder by Delta. In other jurisdictions (cough USA cough), it appears that the apparent increase of kids with severe cases is just because there are more cases, period. Hospitalizations in kids are still really low, and they promise that they are watching really closely.

DrH also emphasized that while the over 70s are very well vaxxed, once a virus gets into a long-term care home, even fully-vaxxed people can get it.
Contact Tracing
They acknowledged that health care services are stretched thin in places. In the Q&A, someone asked if contact tracing was adequate. DrH replied that:
- They are still committed to doing tracing and follow-up for every positive test.
- They are doing less rigorous tracing and follow-up for people who are vaxxed.
- They are moving some people back into contact tracing who had been working on the vaccine clinics.
- Instead of seeing 20 or 30 people getting sick at a party, they are seeing more like 5 or 6 who get sick, that makes the contact tracing easier.
Dix made a comment in the context of contact tracing that the vax uptake was pretty consistent across the province for the older cohorts, that the difference in different areas was really in the under-50s.
Modelling
They said that Rt is falling, but it’s still slightly over 1 and needs to be less than 1 to get the pandemic to fade away. (BTW, Rt in the Interior HA is right at 1.00.)
DrH showed what the models showed for the second and third wave and how, because we took measures, the reality was much lower case counts than expected. She then showed what the model showed for the fourth wave, and how reality was much worse than expected, which she blamed on there being higher contact rates in less vaccinated people in the interior than expected “which we couldn’t have predicted”. (And of course other people did.)
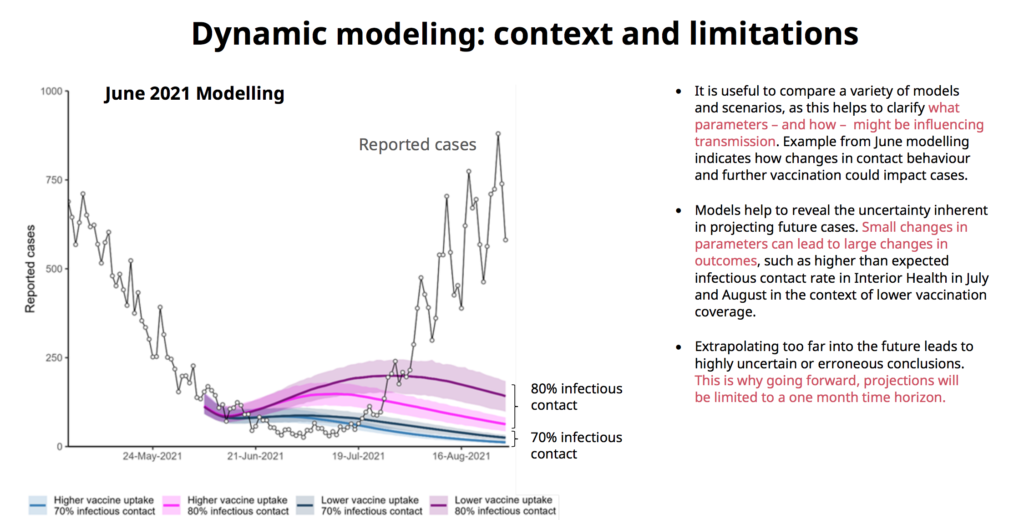
She also made a veiled compliment to what I presumed was the BC COVID-19 Modelling Group, saying that she really liked seeing the modelling that other people did, as different initial conditions could really change the outcomes. (Note: it is true that the province’s models were way over-optimistic in this wave and that the BC COVID-19 Modelling Group did a much better job, I’d like to remind people that the Modelling Group was overly pessimistic on waves 2 and 3. Sometimes ya win, sometimes ya lose.)
One slide showed their model with moderate contact rates, and while hospitalizations increased, they didn’t reach the previous max:

Vax Card
Dix and DrH said that the announcement of the vax card (which really means announcement that you gotta have one to go places) had led to a significant boost in vaccinations. (Meanwhile, yesterday the number of vaxxes was very very low!)
A reporter said that a lot of health care workers in long-term care homes were planning on quitting (because they didn’t want to get vaxxed) and getting a job in a health care setting (like a hospital) where they would not be required to get a vaccination, and asked if the province was going to put in vax mandates elsewhere. DrH said absolutely, Dix said that they were negotiating with the unions.
Schools
DrH took some questions about schools, basically HOW ARE YOU GOING TO KEEP THE KIDS SAFE?!?!? DrH said basically, “look, what we did last year worked and we’ve done ventilation upgrades plus adults are vaxxed so we’ll be fine, tho we will expect an increase in communities where there is high transmission”. She didn’t mention anything about how Delta is lots more contagious. I guess we’ll find out soon enough if the ventilation upgrades were adequate.
She also mentioned that there is extremely high vax rate among teachers. They said, but I didn’t write it down — I think it was like 95%.
She also said that they wouldn’t notify parents if there was just one kid. (She said they got feedback that the parental notices gave more anxiety than useful.) She said they would send notices if there was an outbreak, but didn’t define what “an outbreak” was.
A reporter asked why, if there were vax mandates for long-term care home workers, there weren’t vax mandates for teachers. DrH said that it was crucial in LTCH, that lots of people died. Schools are not as critical, so they didn’t feel they needed such a more proportional approach.
Boosters
There was a question about boosters. While they did not 100% definitively promise that they absolutely will, it’s pretty clear they are planning to give a third dose to certain classes of immunocompromised people, e.g. those with solid organ transplants and some blood cancers. (DrH noted that a third dose helps about 55% of them, so it’s not a panacea.) They are drawing up plans for how to give boosters to people in long-term care homes, but they are not seeing waning vaccine effectiveness, so will hold off until if/when they do.
They noted that most people in BC had longer interval between dose1 and dose2 (6-12 weeks), while in Israel and the US, they stuck pretty closely to a 3-4 week interval. The longer interval seems to give more durable protection. At some point, DrH speculated that the best interval between dose1 and dose2 is probably about six months.
They are also watching the vax manufacturers to see if they deliver boosters tailored to different strains.
Biweekly Data Summary
The Biweekly Data Summary is out, but doesn’t say a whole lot that wasn’t said in the briefing.
- Positivity is high in Interior Health (16%) and Northern Health (20%).




Now, this positivity maps is strange: it covers 18-24 August, while the first map above in the Briefing section covers 15-21 August, and the map above shows 15-20 cases per 100K, while this shows a positivity rate of zero. Maybe this is a small absolute numbers problem?

Statistics
Today: +655 cases, +2 deaths, +4,729 first doses, +6,022 second doses.
Currently 187 in hospital / 103 in ICU, 6,045 active cases, 157,941 recovered.
| first doses | second doses | |
| of adults | 85.0% | 77.6% |
| of over-12s | 84.3% | 76.5% |
| of all BCers | 76.7% | 69.6% |
We have 319,142 doses in fridges; we’ll use it up in 19.9 days at last week’s rate.
We have 271,848 mRNA doses in fridges; we’ll use it up in 16.9 days at last week’s rate.
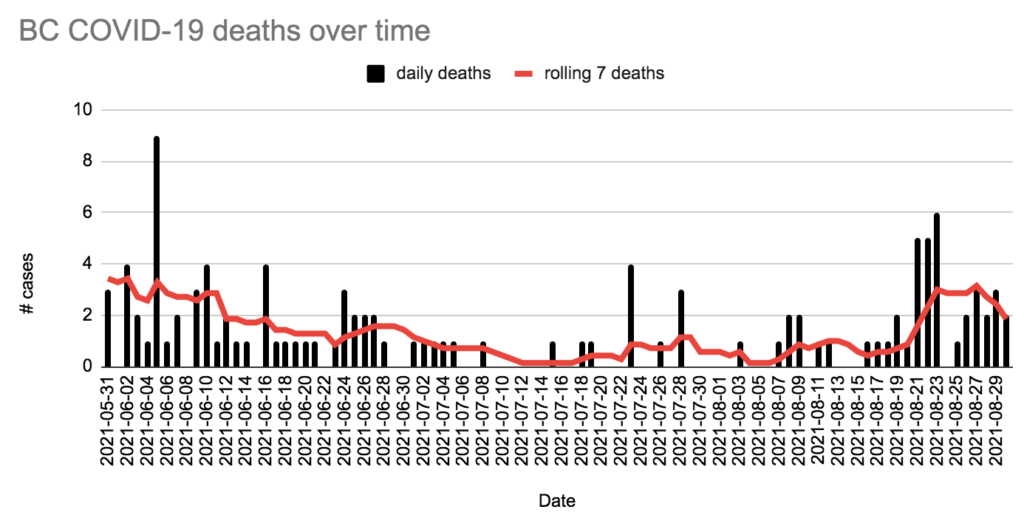
Charts
This tweet had this graph: