Press Briefing
I found the briefing kind of dull. Much of it was slides with information that was already posted in the Weekly Data Summary. Go read that, you’ll get most of it.
The headline is that we’re doing well: case counts and hospitalizations are going down, deaths are low and stable, and we’re vaxxing like crazy. Yes, there are places where case counts are higher, but they are coming down everywhere. Yes, there are places where vax rates are lower, but they’re working on it (and no place is less than 50% vaccinated).
This being a health briefing, they took care to remind us that we are not out of the woods yet, there is still transmission; we have to keep Doing the Things. But Henry and Dix both said that things are looking good.
The most exciting thing was the chart of the reproductive ratio:

R is below 1.0 in all health regions, and I think they said that was the first time since the pandemic started that it had been below 1 in all regions at the same time.
This slide was interesting (and not in the Weekly Data Summary):
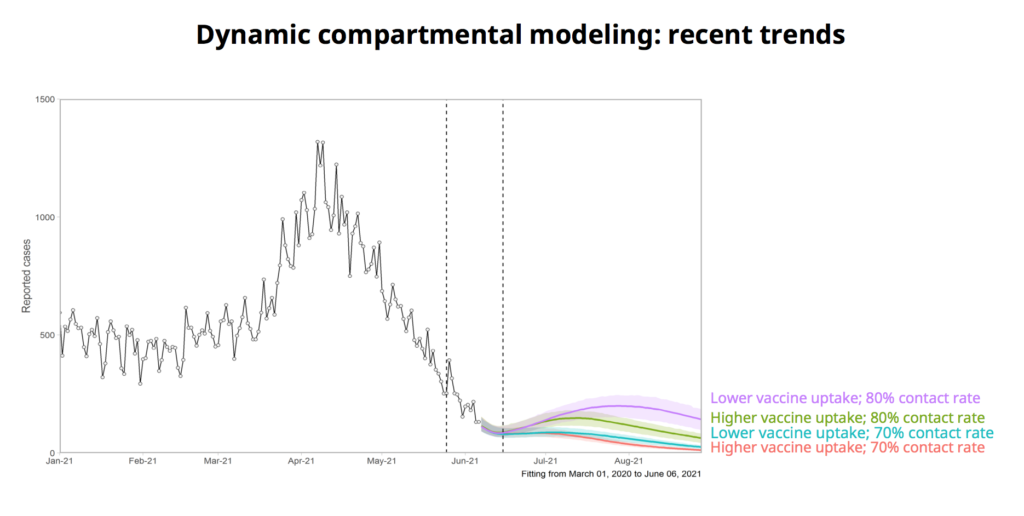
It says that even if we don’t Do All The Things right, we’ll still be okay, and that regardless of what we do, we’re likely to see a small bump in cases soon. One of my associates pointed out that the move to Stage 2 requires falling case counts/deaths/hospitalizations. If we see a little bump on June 15, will we go on to Stage 2, even though overall things have been falling?
Things Dr. Henry said, sometimes in passing:
- Invitations for your second dose will go out after eight weeks, and it might get booked for 1-3 weeks after, especially while we are clearing out the backlog of all the people now eligible. Don’t worry — this dose interval is well within the safe interval for everyone. There’s even data which says that a 12 week delay was 3.5 times better.
- We are still supply-limited. We just got some good news about Moderna giving us a buttload more (though the deliveries are not scheduled yet).
- They are doing whole genome sequencing of every single positive test now. (And by the way, delta is running at about 4% of cases right now.)
Dix spewed statistics, as he does. Lots of vaxxes, hospitals are all fully back from the surgery pause, register, book, vax, etc.
One thing he said was that even though COVID-19 cases are down, the hospitals are super-busy. He did not say why they were super-busy, though, leaving me to wonder. Overdoses? Long COVID? Gang warfare?
Q&A
Continual reminder: snark and heavy paraphrasing ahead.
Q: You said that it looked good for moving to Stage 2, but what does “low” mean for moving from Stage 2 to Stage 3? That’s kind of vague. A: Yes, it’s vague because we need some discretion. Really it needs to be low enough that we can manage it. One outbreak of 30 people is a lot easier to manage than 15 outbreaks of two people.
Q: Are you thinking about making vaccination mandatory for people who work in long-term care homes? A: We think about lots of things, yes, including mandatory vax for workers in LTCH.
Q: Are you thinking about making vaccination mandatory for people who work in long-term care homes? A: Yes, we are thinking about it. But there won’t be any changes before 1 July.
Q: What are you doing to prep for respiratory season in the fall. A: The same thing public health has done for a million-six years: manage outbreaks.
We also are looking at, well, what do we want to keep from the pandemic? Like, we had zero influenza last year, and that piece was awesome. Can we keep it that way?
Dix: There are a bunch of things which we did in long-term care homes. Some of them, we’d already started, some we foisted upon us as part of the pandemic, but quite a few we want to keep. Like the single-site program, which was hugely painful, is definitely worth it. Like we’re investing a lot of capital into LTCH, e.g. to move away from multi-bed rooms. People shouldn’t have to share a room. Not only is it bad for spreading illness, these are people’s homes!
Q: The provincial vax rate is climbing, but there are some places behind like Richmond. Why is Richmond behind? What are you going to do about it? A: We are doing all kinds of different things tailored to the individual area. What works in one place might not work in another. So for example, extended hours can help in places where people have long commutes like Mission. Mobile clinics like we’re doing in the Interior can help rural areas. Pop-up clinics have been successful in Surrey, but maybe in Cherryville it needs to be at Frank’s Grocery. Across the board we’re working with faith leaders and community leaders.
Dix: And if you look at Richmond, they are now above the provincial average in registrations thanks to a lot of work by a lot of people. It will take a little bit for that to show up in the vax numbers, but it’s coming.
Q: Y’all say that things are going great, what could screw things up? A new scariant? A: Things are going great in large part because the vaccines are just so fucking awesome, and the first-doses-first policy is really paying off. We hope that the vaccines will last until next fall (2022, I think DrH meant, because it’s clear they will last until September). We could get a new scary variant, even a home-grown one, but that’s unlikely as our case counts go down. What we really need to do is get our case counts way down before the fall respiratory season, so we don’t have to deal with a lot of COVID-19 on top of the normal influenza, enteroviruses, RSV, etc.
We need to keep our eye on the global picture, but the way we prepare is by beefing up our public health capabilities, like our whole-genome sequencing capabilities.
Q: How close are we to vaccinating the under-12s? A: Moderna has already submitted data for the under-12s. Both Pfizer and Moderna have started studies all the way down to six months. Pfizer is looking at lower doses for younger children. Those studies should be done by October, so vax should be available by the end of the year.
Also, there is some really good data that says that vaxxing adults helps protect the kids. (See today’s General blog post for more.) Reducing the case rate helps everybody.
The under-12s are about 11% of the population, so we can get really high vaccination rates even without them. Globally, it’s important to vaccinate health care workers and adults around the world, then look at how to protect children individually. (I think she just called for sending vax overseas before giving it to our children.)
Q: Should we be doing more 24/7 clinics? A: That doesn’t make sense everywhere. Dix: The problem is not clinic hours, it’s supply. Last week we were virtually out of Pfizer. When we have more supply, then we can expand the clinics.
Q: Some ppl who got an mRNA want same vax for their second dose, can the system be updated to show what vax a clinic has on that day? A: No. It’s a big system with lots of moving parts. We will try — and that will get lots easier once we get the big Moderna shipment — but chill, Pfizer and Moderna are nearly identical. You’ll be fine.
Q: How do we “live with COVID”? A: We handle it like other infectious diseases, which pub health does All. The. Fucking. Time. We treat it like measles, like pertussis. We do rapid tests, like we do with influenza. We test/trace/track.
Statistics
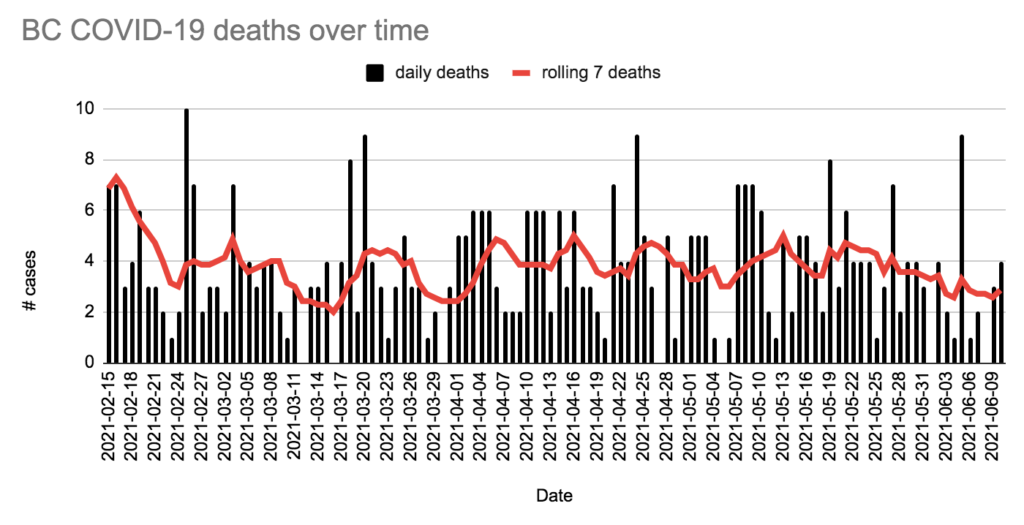
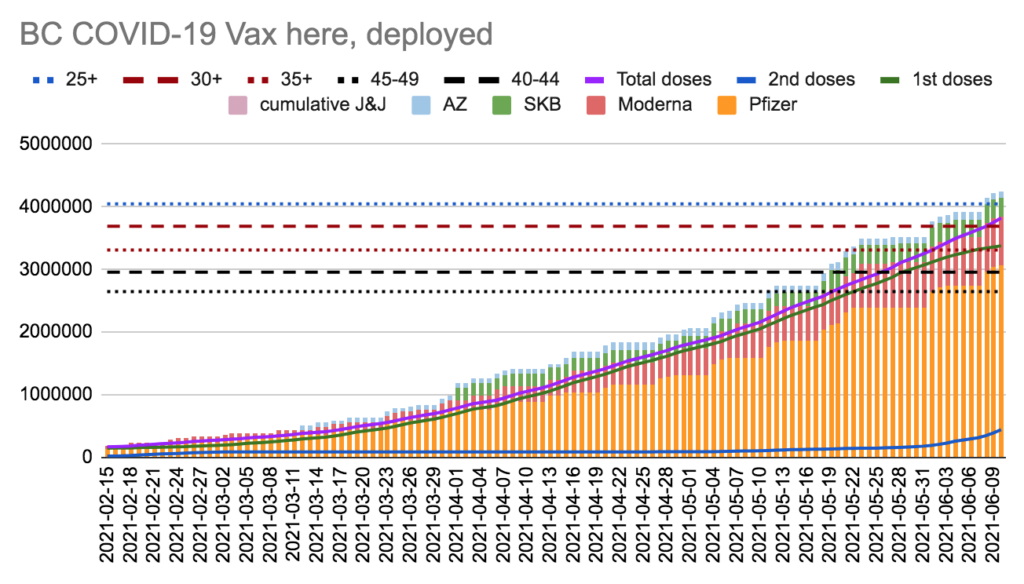
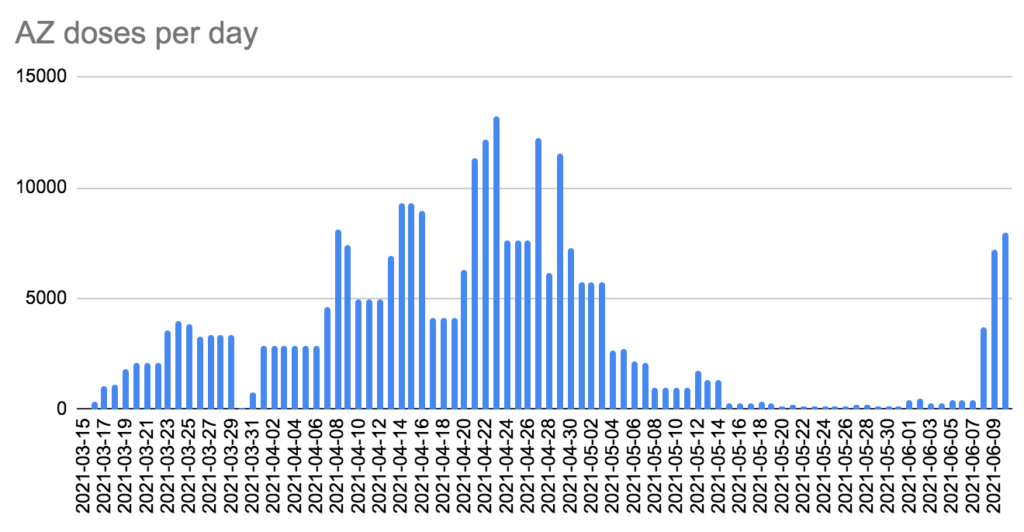
Today: +153 cases, +4 deaths, +8002 AZ doses, +20,047 first doses, +53,298 second doses.
Currently 176 in hospital / 49 in ICU, 1910 active cases, 142,314 recovered.
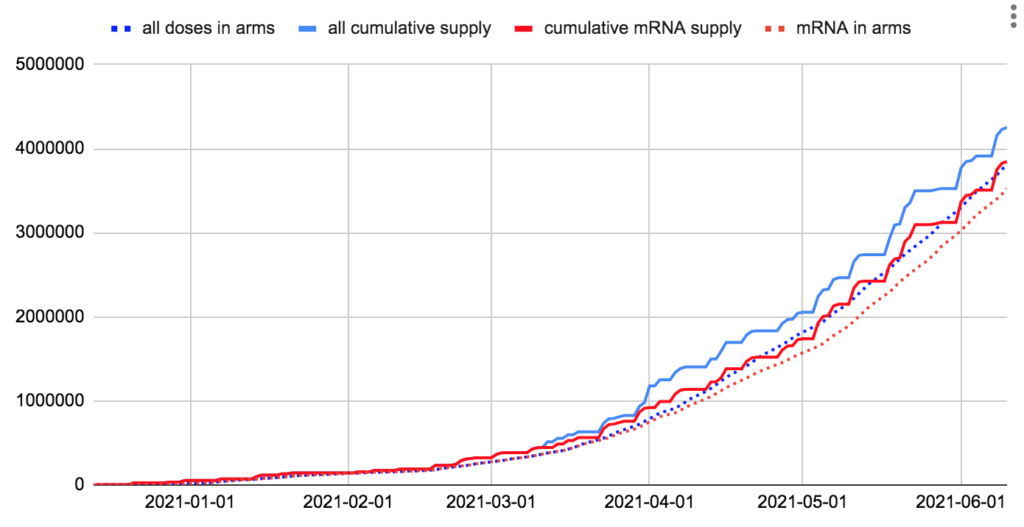
We have 429,627 doses in fridges; we’ll use it up in 8.0 days at last week’s rate.
We have 403,900 mRNA doses in fridges; we’ll use it up in 7.1 days at last week’s rate, ulp.
We have 105,335 AZ doses in fridges; we’ll use it up in 13.2 days at yesterday’s rate.
Charts