The news has been slow, I think in part because the US has a long weekend, but also because COVID-19 is generally receding as a major issue, certainly in the US but also somewhat in Canada.
Variants
On Thursday, Dr. Henry nonchalantly announced that they were dropping the dose interval from 16 weeks to 8 weeks. This surprised me slightly; I had expected that we’d switch over around the 15th. I was even more surprised that my 80-something neighbour got an appointment right away, for today. So it’s not that they waited until demand for shots was low to switch over to second doses. No, they decided they wanted to get second shots in arms, and to do so right away.
I think the math has changed with B.1.617.2 (“India”). While the effectiveness of 2 doses is less than twice the effectiveness of 1 dose for all the other variants, it is not true for Pfizer against B.1.617.2: one dose only gives 33% effectiveness and two doses gives 88%. Given that old people are much much more likely to need hospitalization and/or die from COVID-19, the math in the presence of B.1.617.2 suddenly switches into GET AS MANY OLD FOLKS THEIR SECOND SHOT AS POSSIBLE, STAT!
Do we have B.1.617.2 in BC? A little bit:
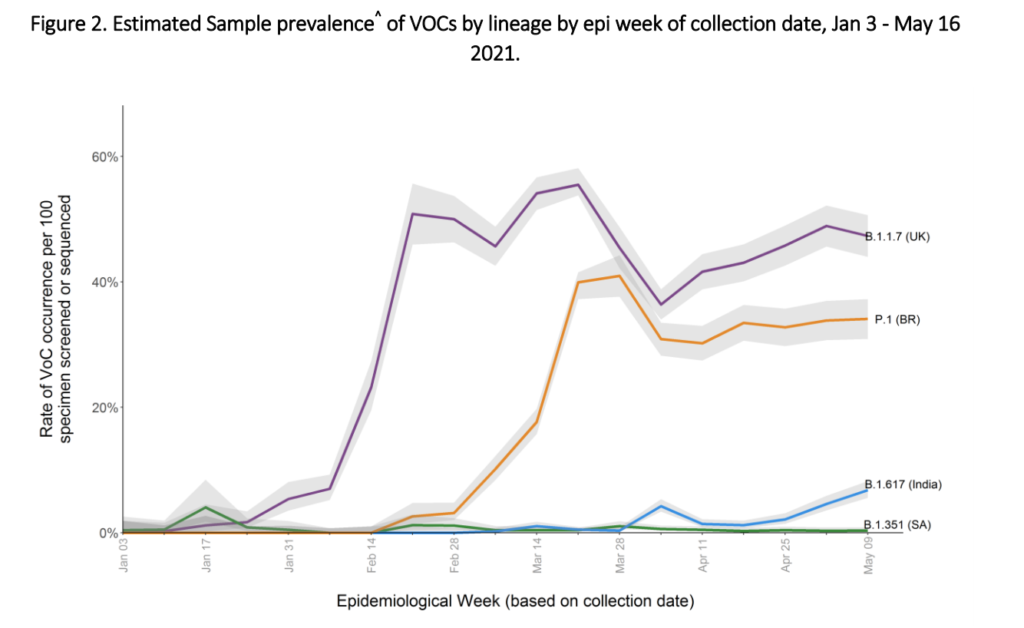
Eyeballing, that looks to me like B.1.617.2 was at about 7% two weeks ago and rising very fast. It would not surprise me if it’s now at 20% or more. This is not good.
I think maybe we reopened too soon.
Press Briefing
Dr. Henry opened with heartfelt words about the tragedy, the abomination uncovered at the Kamloops residential school. I cannot do the words justice, I cannot write a summary because I cannot summarize an emotion. Watch the video.
After those remarks, Dr. Henry said:
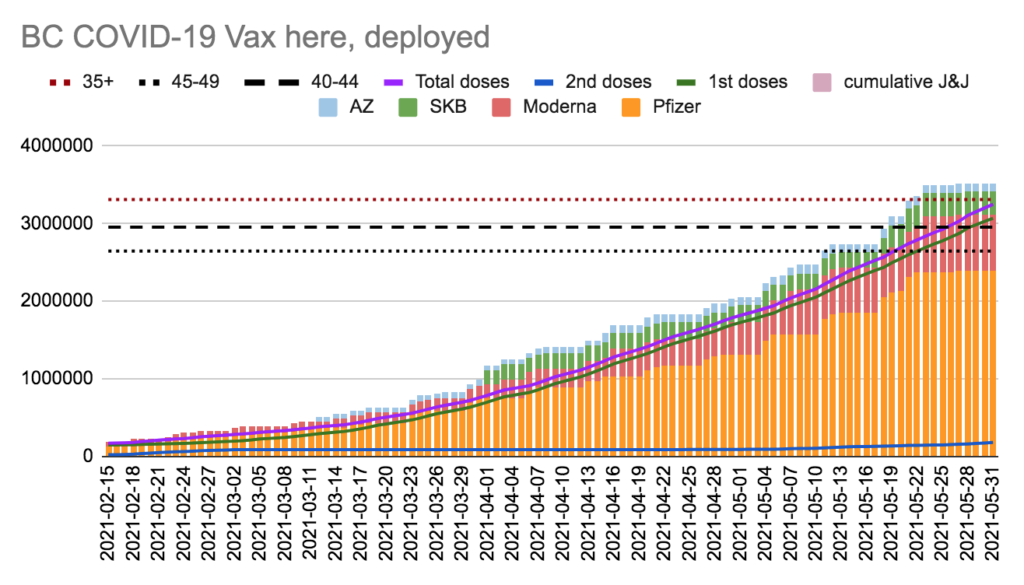
- 69.7% of adults and 66.1% of those over 12 have been vaccinated, woohoo! NB: This is about 60% of all BCers.
- BC has seen its third case of VITT (AZ blood clots), in a man in his 30s. He’s in hospital getting treatment and recovering.
Dix said:
- Sadness over the Kamloops children. He gave several phone numbers:
- Anyone who experienced racism in healthcare can share their experiences at 1-888-600-3078
- national residential school crisis line set up to provide 1-866-925-4419
- 1-800-588-8717 BC-specific crisis line
- Today, only 7 surge beds are being used, which is a big improvement. COVID hospitalizations are way down from a high of 511 to 249 today; COVID ICU patients are down from a high of 183 to 78 today. However, the hospitals still have a high number of patients. NB: Once patients test negative for COVID-19, they are no longer included in the hospitalization numbers. This isn’t as underhanded as it might look at first, because it really matters to the hospital how many COVID-19 positive people they have. People who are COVID-19 negative can be transferred to non-COVID hospitals, for example. It is my understanding that people who are admitted to the ICU are still counted after they are COVID-19-clear.
Q&A
Q: Manitoba decided they were tired of waiting for the UK mix&match study of AZ/Pfizer and are just going for it, giving Pfizer to Team AZ. What is BC going to do? A: The UK study is late, but there is other data out there that we’re looking at. People will have a choice, but we need to figure out the messaging and the logistics. I’ll let you know on Thursday. NB: I think that she meant things like, “how do we modify the registration system to give people the choice?” Another possibility is that they are figuring out what dosing interval to use.
Q: Will Team AZ be able to get AZ+Pfizer+Pfizer if they need two Pfizers for proof of vaccination for travel? A: Uh, that shouldn’t be a problem. AZ+Pfizer should work better than AZ+AZ, and if somehow it’s not as good, we’ll get you a booster.
Q: I heard that people’s vaccine appointments were cancelled once they got there because there just wasn’t enough vax. WTF? Was it just a bunch of kids showing up without appointments with their parents? A: That’s news to me. Some people got their appointments cancelled because it turned out there hadn’t been 8 weeks from their first vax. There was also an issue with blank screens over the weekend because of system maintenance, sorry about that. But I haven’t heard about supply problems.
Q: WHY CAN’T I TAKE MY MASK OFF WHEN VISITING GRANDMA IN THE LONG TERM CARE HOME??? A: Because it’s still dangerous. Vax doesn’t always work, not everybody is vaxxed. Assume you’re still going to have the current restrictions until July.
Q: As more teens get vaxxed, can you imagine policies which allow vaxxed teens to have more comprehensive ceremonies? A: The School Health Team is considering options.
Q: Oh come on pleeeeeese? Graduation is sometimes the last week in June, which is RIGHT before July 1, which is when Stage 3 should kick in, can’t they pleeeeeeease get a variance? C’mon, you gave a variance to religious groups! A: The School Health Team is considering options. NB: I am impressed with her ability to NOT say, “Like I just told you 15 seconds ago…”
Q: Last week you said that the clinically extremely vulnerable people would get priority for dose #2, what about the people who are not on the CEV list but who are really vulnerable? A: We made the list pretty broad for people who are at risk. There are a fair number of vulnerable people who are not at higher risk for COVID-19. NB: This is true. Multiple sclerosis, for example, does not increase someone’s risk of COVID-19 although a few (not all!) of the MS immunosuppressive medicines do. Also, nobody is excluded, everybody has to still take measures — so if you are immunocompromised, you still need to protect yourself. Also also, everybody is going to get doses and we are going really fast now.
Q: How are we going to make sure that restrictions are rolled back uniformly across the 500+ long-term health care homes? A: It’s a challenge, but it’s too early to roll back restrictions.
Q: How many teens got Moderna instead of Pfizer? A: About a dozen. That was absolutely an error, our bad, but it shouldn’t actually hurt them. Moderna has submitted the results of their trial on 12-17 year-olds, and we expect that it will get approved very soon. Still, it was bad and we have instituted some procedures to make sure it doesn’t happen again.
Q: One dose is really crappy against B.1.617.2 but two doses works well. Should we worry about B.1.617.2? A: That was a really small study. NB: It wasn’t THAT small: there were ~12K B.1.1.7 people and ~1K B.1.617.2 people. At the population level, we’re seeing cases still go down in the UK. We use vax level AND cases AND deaths. We need to keep those in a range where pub health can do test/trace/track properly.
Statistics
Fri/Sat: +258 cases
Sat/Sun: +238 cases
Sun/Mon: +212 cases
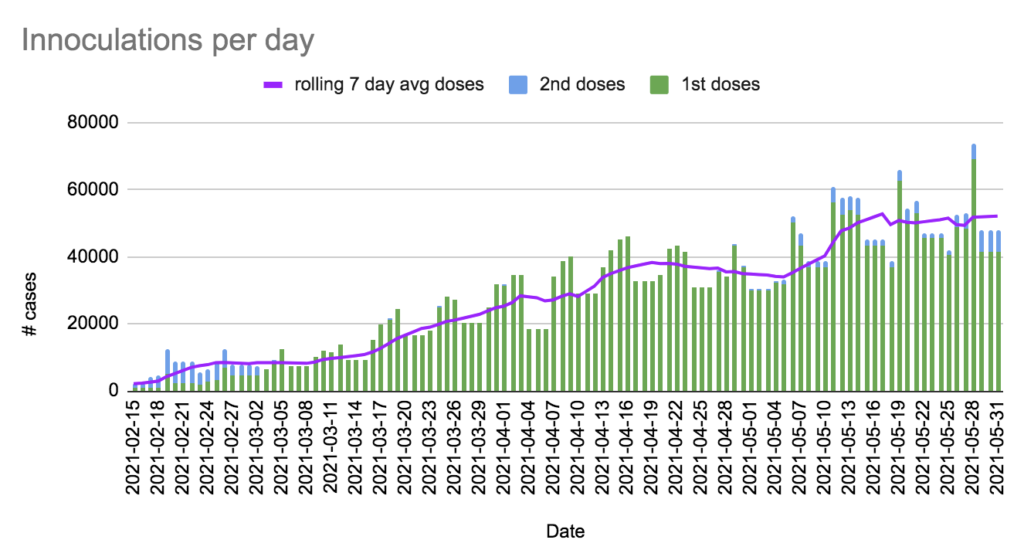
Over weekend: +11 deaths, +124,778 first doses, +19,069 second doses. The ages of the deaths were as follows:
| Age cohort | # of cases |
| 40s | 1 |
| 50s | 0 |
| 60s | 2 |
| 70s | 6 |
| 80 and over | 2 |
Currently 249 in hospital / 78 in ICU, 2953 active cases, 139562 recovered.
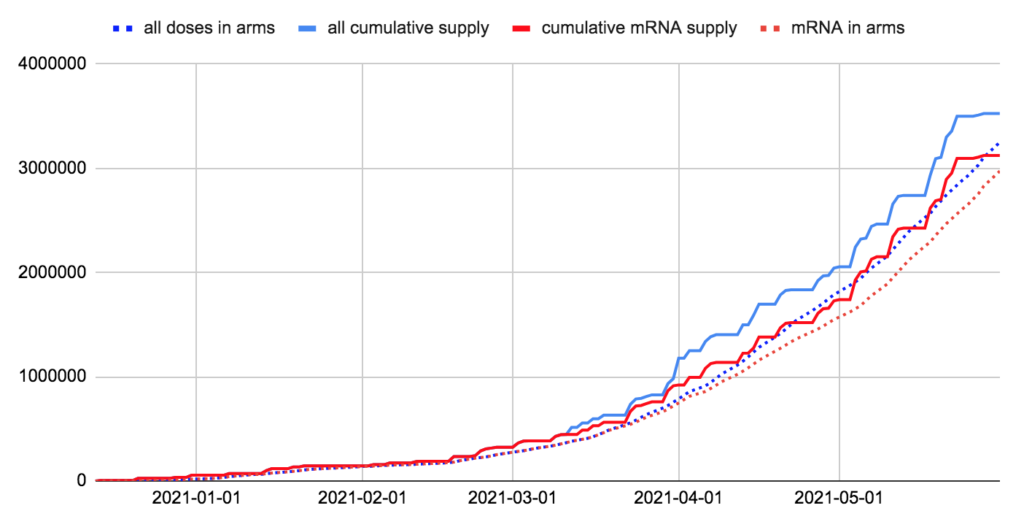
We have 276,214 doses in fridges; we’ll use it up in 5.3 days at last week’s rate. We’ve given more shots than we’d received by 11 days ago.
We have 149,183 mRNA doses; we’ll use it up in 2.9 days at last week’s rate. We’ve given more mRNA shots than we’d received by 9 days ago.
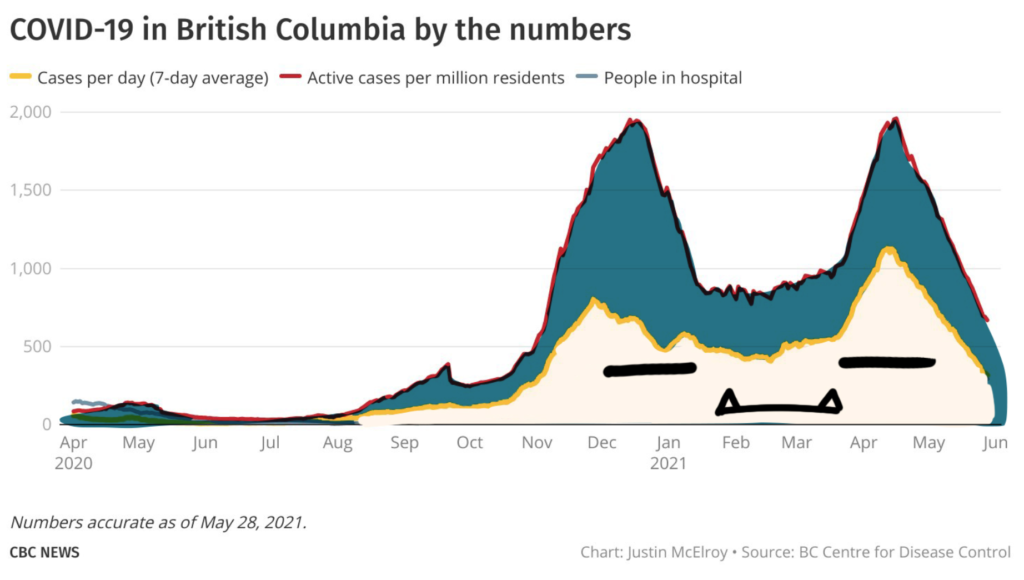
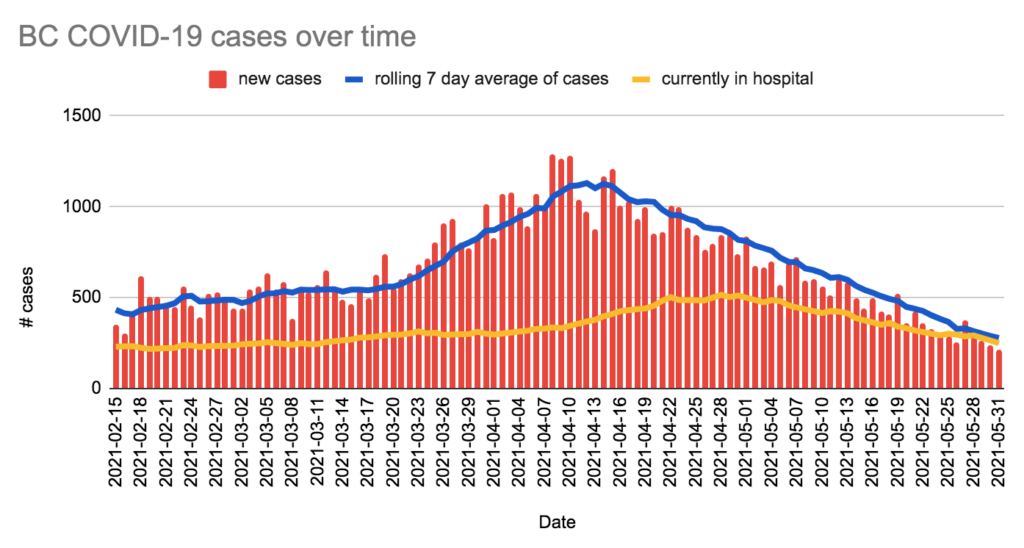
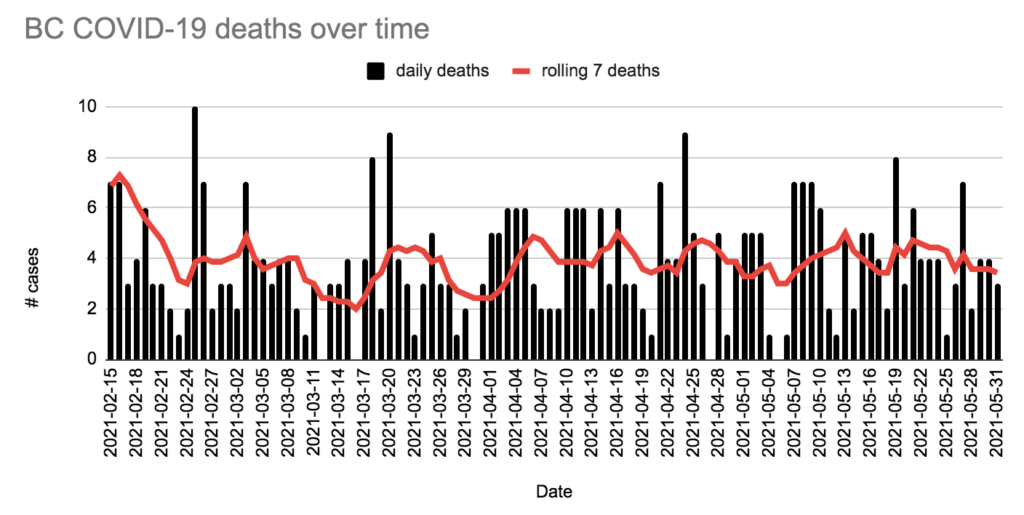
Charts
Humour
This is a few days old, but I realized some of y’all might not have seen it: