
Variants
I have been frustrated with some of the talk around Omicron’s virulence, and this tweet made me realize what my problem was: we shouldn’t be talking about THE virulence (usually expressed as the Case Hospitalization Rate or CHR) as a single number. There is a different CHR for the general population (the observed virulence) and the CHR in unvaccinated people (the intrinsic or innate) CHR.
Both are important. Knowing what the observed CHR is very very important for people who are making predictions about if when the health care system will collapse. But knowing what the intrinsic CHR is is really important for individuals who are unvaccinated or immunocompromised. (And of course, those of us who are vaccinated want to know what the CHR for people vaccinated with our exact brand of first dose and our exact brand of second dose and how that varies over time, but that’s asking too much…)
It gets even more complicated when you try to figure in prior infection, because infections are pretty grossly under-counted. (Infection alone gives less protection than vaccination alone, but infection+vaccination gives the best protection against further infections)
Most of the studies that are out there are only give information about the observed virulence. Given that the best data we have right now is from countries with high immunity to prior strains (South Africa from infections, Denmark from vaccinations, UK from both), it’s really really hard to tell what the intrinsic virulence is.
The observed virulence of Omicron seems to be somewhere between 20% and 60% of the virulence of Delta. This wide range is reasonable, seeing as how the different geographies have wildly different age and economic demographics, vaccination histories, prior COVID infection histories, etc. However, the one paper which tried to figure out the intrinsic CHR found that Omicron’s intrinsic CHR wasn’t much lower than Delta’s.
REGARDLESS, it… doesn’t matter. Even if Omicron’s CHR is only one-fifth of what Delta’s CHR is, if you have ten times as many people going to the hospital, you still are going to overwhelm the hospitals. PEOPLE ARE GOING TO DIE. LOTS OF THEM. Those photos of refrigerated trucks to hold the bodies because the morgues are full? That’s going to happen in Canada. In the suburbs, there are going to be more cars in the streets because people are going to put dead bodies in the garages while they wait for hospital space.
The time to panic is now! Don’t go to that big dinner party! Hide in your home!
More Details
You might not care, but dammit I spent a lot of time reading these studies and want you to realize why I didn’t report on much else today.
The best data comes from these four studies from four places:
The report from Denmark is just numbers, with no statistical analysis. I’m not going to do the analysis. But here’s a picture (from this tweet) (though I think they have the colours backwards):

The report from England tried very hard to figure out what the intrinsic vs. observed virulence was. They adjusted for age, sex, ethnicity, region, date, and other socioeconomic factors, then also for vaccination status.
- The observed CHR of Omicron is about 55-60% of that of Delta when defining hospitalization to be a stay of a day or more (i.e. just visiting the emergency room wouldn’t count).
- If you have had a COVID-19 infection, you are almost 70% less likely to go to the hospital for a day than if you were not infected (assuming 3x undercounting of prior infections).
- Once you have an infection, if you had two doses of mRNA, the risk of hospitalization is about the same for Omicron and Delta.
- Once you have an infection, if you had two doses of AZ, the risk of hospitalization is slightly less for Omicron compared to Delta.
- The asterisk* in the previous two bullet points is because it might be that your risk is the same whether you got mRNA or AZ because mRNA is better at keeping you from getting infected.
- With the assumptions they made about how many people had prior infections, they calculated that the intrinsic virulence was only slightly less for Omicron than for Delta.
- There is some indication that hospital stays are slightly shorter for Omicron than for Delta (0.22 days vs. 0.32 days)
Here’s a Twitter thread discussing the England report in detail.
The report from South Africa says:
- The observed CHR for Omicron was only 20% of the Delta CHR but
- they compared two different time periods for their Omicron/Delta comparisons, instead of the same period with Omicron/Delta determined by testing (while the England paper did) and
- they did not account for the huge seropositivity rate (like 70%).
- People who were hospitalized with Omicron were about as likely to go to the ICU as those hospitalized with Delta.
The report from Scotland says:
- The observed risk of being admitted to a hospital from Omicron is one-third that from Delta.
- I don’t know what “admitted” is for sure, but I don’t think emergency room visits count.

In a rare piece of good news, this article reports that case counts are falling in South Africa. This tweet points out that South Africa, Denmark, and Norway are all seeing quick declines:
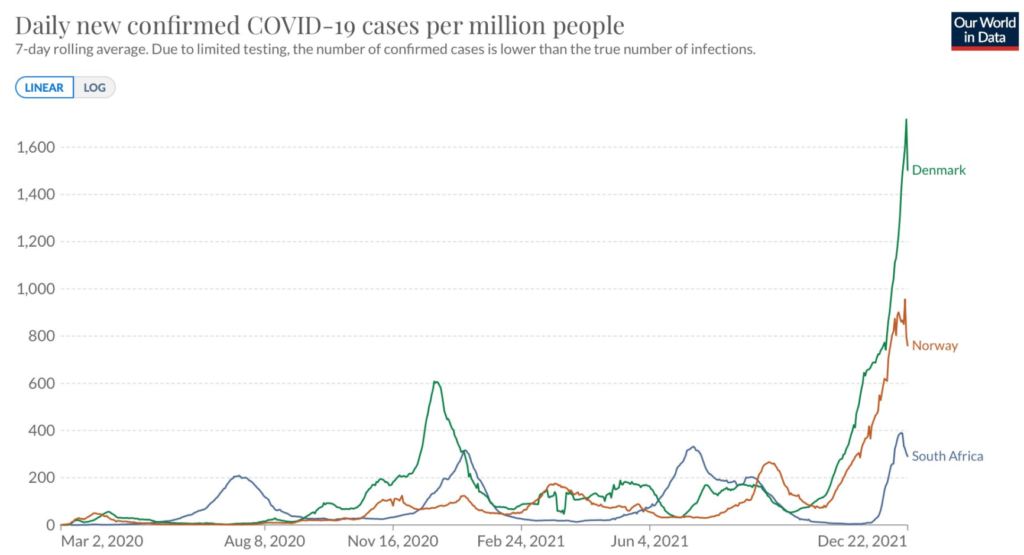
Nobody has any idea what a mechanism for such a quick decline could be, so it’s premature to count on it happening here.
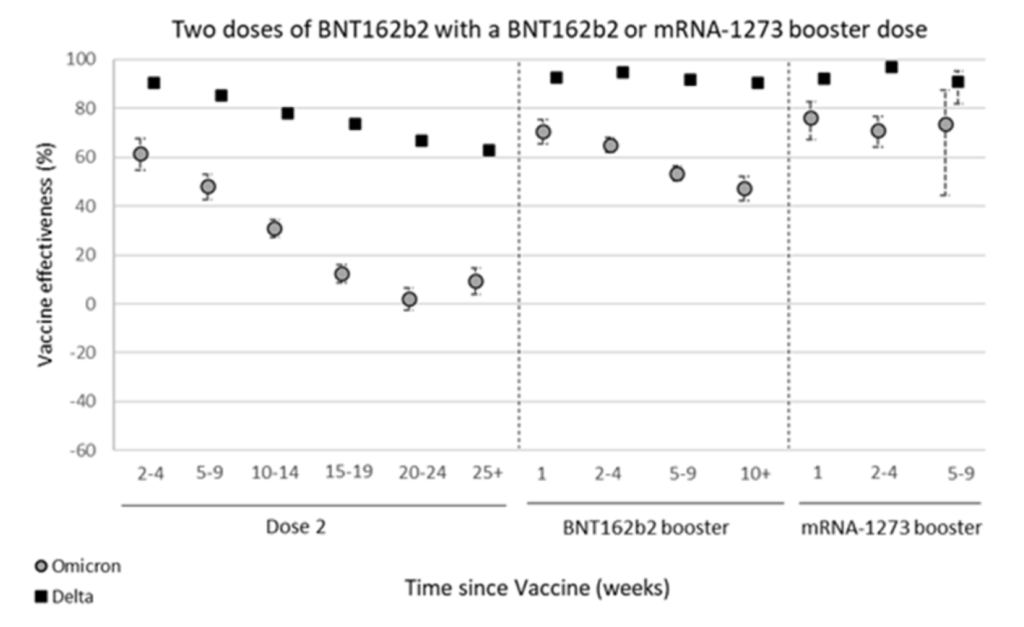
This report says that waning against Omicron is even more pronounced than waning against Delta:
Treatments
Hey! Good news! This preprint says that high-risk patients who took remdesivir within seven days of a positive test were 87% less likely to be hospitalized! Now, remdesvir is an infusion and not a pill like Paxlovid, but three days of infusion are still better than twenty days on a ventilator.
Modelling
The Institute for Health Metrics and Evaluation forecasts a little over 200K cases PER DAY in Canada at the end of January. (BC’s share is 27K cases per day.)
Recommended Reading
This article (by THREE of my favourite authors!) forecasts how the US’ response is going to be inadequate in the face of Omicron.