
Vaccines
Today, during a BC Ministry of Health press conference about something else, Dr. Henry got a question about when little kids’ vaccinations (ages 5-11). Dr. Henry said that Pfizer had submitted (or was about to submit?) data for the study, which had a new formulation: 1/3 of the adult active ingredient (10 mg vs. 30 mg) and which was fridge-stable. She was enthusiastic about it the new formulation being fridge-stable, but I was going “Waitaminute! Does that mean that we have to order special kiddie doses instead of just using 1/3 dose of the TEN MILLION adult doses we have in the freezers?” I hope not.
I can imagine Health Canada saying, “Welllll we know Pfizer says that it needs to be a new vax, but we know it reeeeally doesn’t matter”, sort of like how Health Canada said, “Weellllll Pfizer says to only use Pfizer for its second dose, but we know Pfizer and Moderna are close enough that you can mix&match them no problem.” I can also imagine Health Canada sticking to its guns and saying, “we do not have data on giving the kids 1/3 adult doses, so we’re not going to allow using adult doses on children”, but I have a hard time imagining Health Canada being able to stand up to the fury of millions of frightened parents.
I wonder if we will get a hybrid: “If you want to give your child an unproven 1/3 adult dose, go for it, but any problems are your fault. If you want to wait the year for the kiddie doses to show up, then okay, wait.”
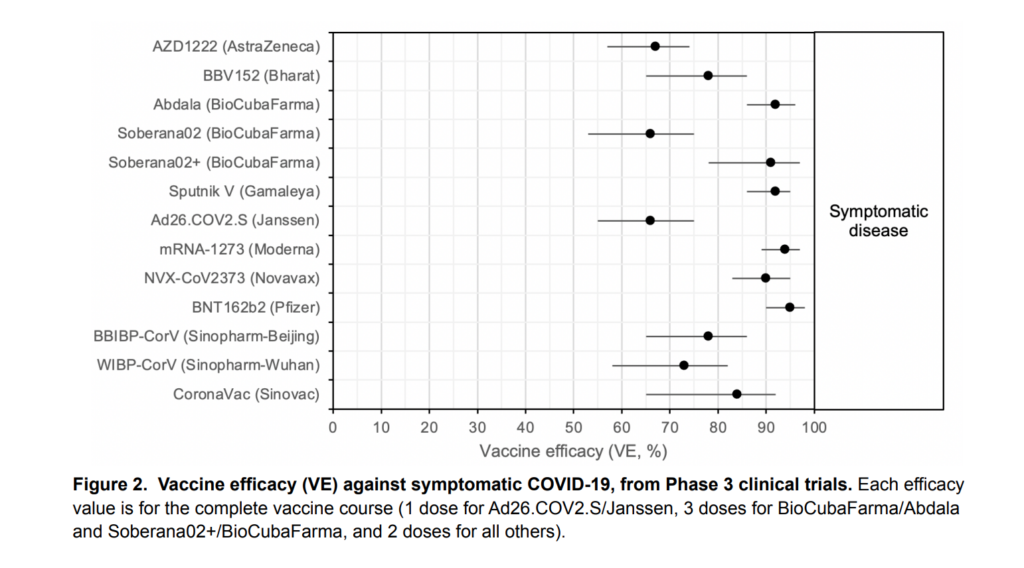
This review article looks at alllll the vax studies for all the WHO-approved vaccines and threw out the ones which were sketch (e.g. relied on self-reporting to tell if someone had prior COVID-19 disease). Here’s the money shot table:
This paper argues that age-based distribution of COVID-19 vaccine was inherently unfair to people of colour because mortality rates in BIPOC are higher than of White people of the same age:

By the way, this article reports that it’s safe and fine to get a flu vax and COVID-19 vax at the same time. So when flu shots become available in two weeks (ish), go ahead and get one.
From this Twitter thread:
Treatments
This article says that trials of Merck’s drug molnupiravir were so good that they applied to stop the study early: it appears to cut hospitalization in half. It works by fucking with the viral replication: it causes so many mutations, so many copying errors that the virus just can’t function.
This is great news, but the Wikipedia article on molnupiravir says that there are concerns about this drug (or others like it) could cause mutations in the DNA of the humans who take it.
It costs about CAD$900 per treatment regime. This article says that about 1 in 14 people who test positive need hospitalization, while this article says that the average COVID-19 hospital stay costs CAD$23,000. 14 people * CAD$900 per treatment / 50% reduced risk from the drug = CAD$25,200, or approximately the same cost as hospitalization before counting the societal cost cost of death and Long COVID (although also not counting the cost of side-effects from the medicine).
The article also said that Merck was working with some companies which normally produce generic drugs, in an attempt to get the cost down.
If this drug does get approved, one thing it might enable is human challenge studies (i.e. when you deliberately infect someone). Right now, most countries consider them unethical because the treatments aren’t great, but human challenge trials are really really useful for a lot of things. For example, how much virus is needed to get you sick via eating, mouthbreathing, nosebreathing? What is the variation in susceptibility, by age, by race, by immunosuppressive category?
Origins
If you’ve been paying any attention to COVID-19 (which you presumably have, because you are reading this), you have seen speculation on the origins of SARS-CoV-2: did it come from a bat directly or did it come from the Wuhan Infectious Diseases lab manipulating a bat virus and then oopsie letting it escape?
Scientists recently found a virus in a bat in Laos which was very very close to COVID-19, but it did not have something called a furin cleavage site. Well, this preprint found that furin cleavage sites occurred independently multiple times in the coronavirus family. That makes it even less likely that SARS-CoV-2 came from nefarious doings at the Wuhan lab.
Recommended Reading
This article looks at how a pandemic ends, with discussion of how a few countries (e.g. Denmark, Norway) are doing as they at least appear to be pulling it off.
This Twitter thread talks about what “endemic” means (and it’s probably not what you think).
This article explains, again, why vaccines are safe.