
COVID-19
Long COVID
This paper from Japan (2026-05-08) reports that Long COVID rates dropped from Delta to Omicron/2022 to Omicron/2024, in both children and adults:
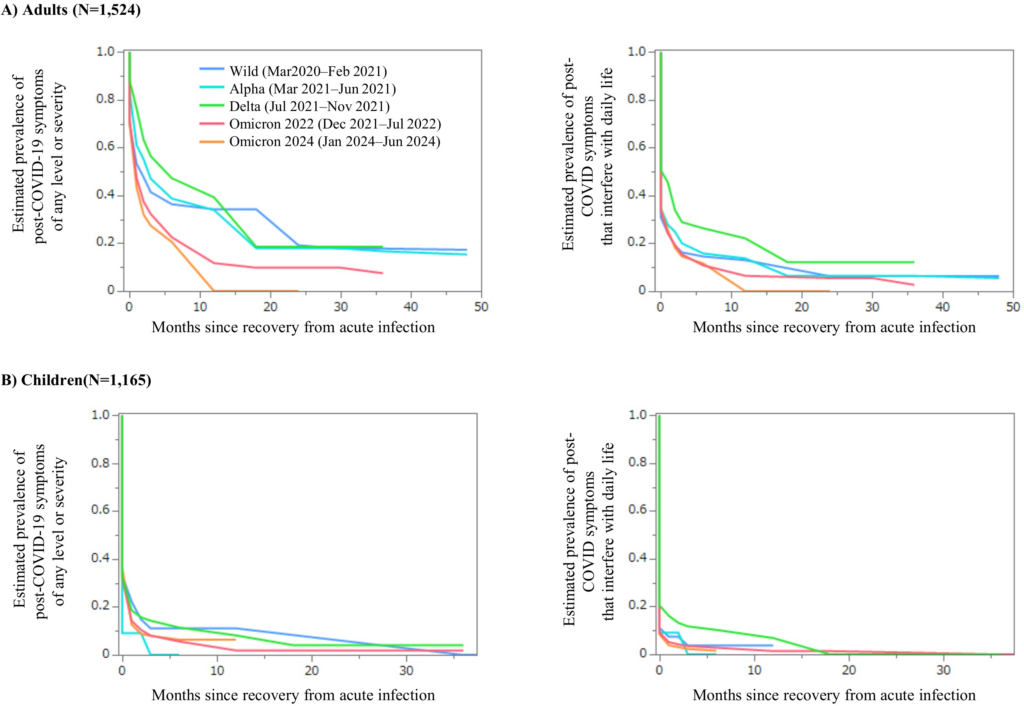
Note that most people with Long COVID symptoms got better relatively quickly, but it then plateaued: if you weren’t better after ten months, you weren’t likely to be better at 50 months. 🙁 This is consistent with my anecdata; I know quite a few people who lost their sense of smell, or had pain, or fatigue, who got better within six months. It would be interesting to see how recovery of different symptoms changed with the variant.
COVID-Related Excess Death and Sickness
🤰This paper from Ontario (2026-05-07) reports that babies born to mothers who had COVID-19 infections while they were pregnant had no higher risk of birth defects. Whew!
Pathology
One thing that my loyal opposition likes to say is that people who died from COVID-19 would have died anyway. This paper from England (2026-05-08) reports that, even for people over 65, they would have been expected to have four or five more years of life if they had not caught COVID-19, and that 28% of them would have lived for more than five years afterwards. For women between 65 and 74, 66% would have been expected to live more than five years more.
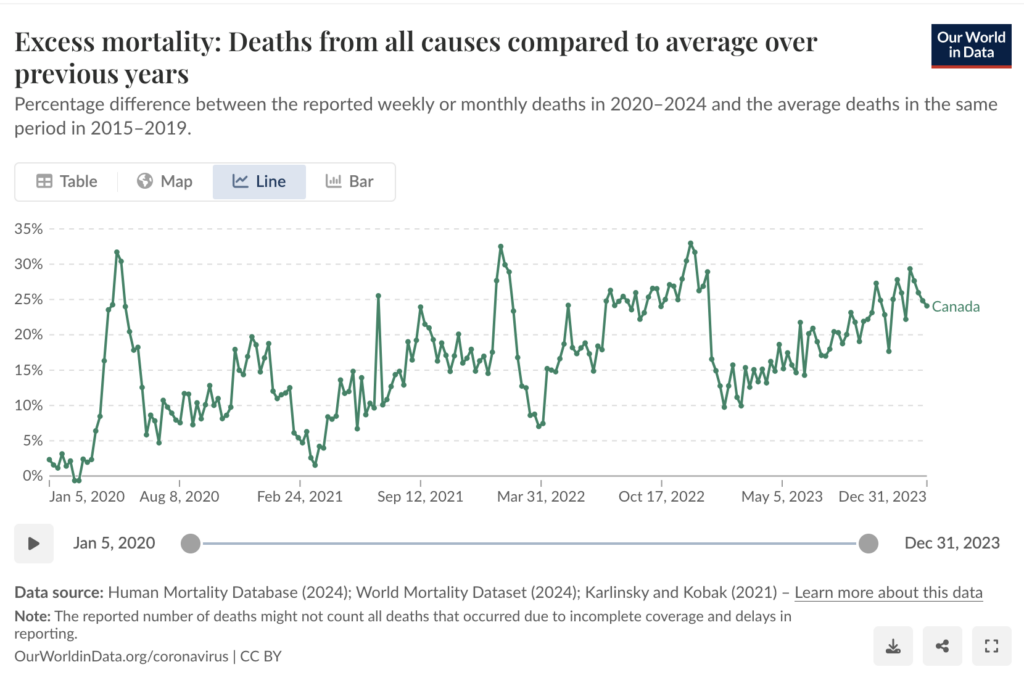
This blog post (2026-05-12) absolutely destroys the “yeah, but the people who died all had comorbidities” argument (using facts!). For example, the excess death rate went up significantly. If “all those people were going to die anyway”, then you would expect the excess death rate to go lower than baseline after a few years because so many deaths got shifted earlier, but the excess death rate went up:
I wanted to see for myself, so I grabbed the data for COVID-19 related deaths in England and Wales between March and 4 July 2020 (because that was what I found quickly), and the share of deaths that were in people under 65 with no underlying conditions was 13.2%. So yes, most of the people were old and/or comorbid, but 13.2% is still a lot of young healthy people!
It might even be more than 13.2%: someone might have a comorbidity, but that comorbidity might not have had any influence on the death. For example, I’m not sure that early stage fatty liver disease or mild epilepsy really would cause you to preferentially die of COVID-19. That would make the true percentage of healthy young people even higher than 13.2%.
This paper from USA (2026-05-08) reports that getting a COVID-19 infection increases the 90-day mortality risk after getting surgery for hip fractures compared to no infection:
| Time of infection before surgery | increased 90-day mortality risk |
| within 6 weeks | +97% |
| within 12 weeks | +69% |
| within 6 months | +29% |
Among patients who got COVID-19 infections, being unvaccinated hugely increased the mortality risk compared to being vaccinated:
| Time of infection before surgery | increased 90-day mortality risk |
| within 6 weeks | +337% |
| within 12 weeks | +336% |
| within 6 months | +349% |
Variants
🐀 I always thought that Omicron probably evolved all its mutations in an immunocompromised person who had an active case for months or years, allowing plenty of time for mutations to accumulate. However, this paper (2022-01-25) suggests that an early variant jumped to rodents, mutated, and then jumped back to humans as Omicron and this paper (2025-10-22) reports that an Omicron variant was in fact circulating in rodents in Mexico in late 2020!
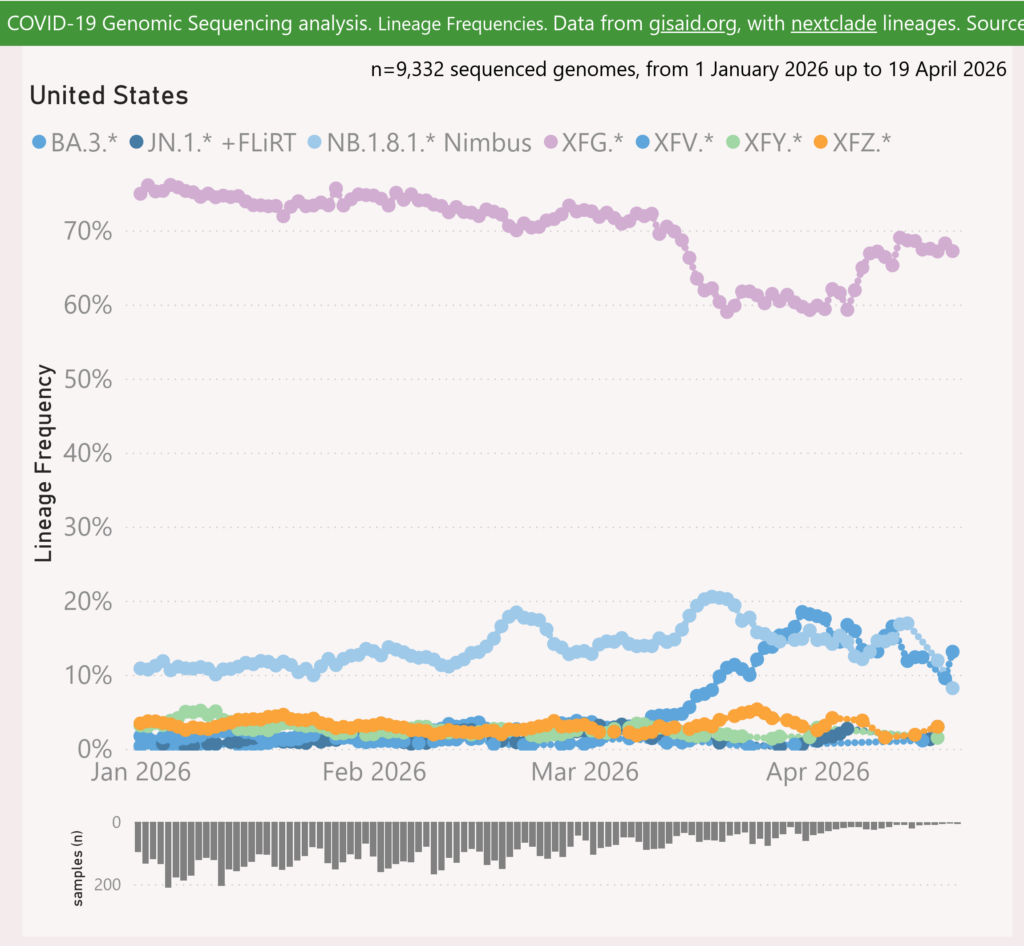
This report (2026-05-12) shows that the share of BA.3.2 (“Cicada”) has actually gone down in the USA. So much for BA.3.2 being a big scary boogeyvirus.
Treatments
🎉💊 This paper (2026-05-13) reports that a Phase 3 study with participants from five countries around the world showed that Ensitrelvir (sold in Japan under the brand name Xocova) reduced household transmission. When someone started having symptoms of COVID-19, if their household members started taking Ensitrelvir within 72 hours, their rick of getting a COVID-19 infection themselves dropped by 66% compared to those taking a placebo!
Vaccines
💉 This paper (2026-05-13) from Denmark reports that the adjusted vaccine effectiveness of the LP.8.1 vaccine against hospitalization was 60·6% and 70.1% against death within 30 days (compared to unboosted people). It did decrease in effectiveness from 66% at 14-30 days after vaccination, down to 48.3% after four months. They could not see a clear loss of effectiveness against death.
💉 Getting vaccinated doesn’t always keep you from getting COVID-19, and it doesn’t absolutely keep you from passing it on if you do get sick, but vaccination does significantly reduce how well you will pass it on. This paper (2026-05-15) from USA reports that household members of someone sick with COVID-19 had a 43% lower risk of catching COVID-19 themselves if the sick person had been vaccinated less than six months earlier (compared to the sick person not having been vaccinated). After six months, a vaccine was no help — so this is a reason to keep getting vaccinated.
Hantavirus (ANDV)
Transmission
This snippet is long. TL;DR: from what I see, you absolutely do not have to have “prolonged close contact” with someone infected with hantavirus to catch it but only a very small percentage of exposed people actually get infected. At this point, asymptomatic transmission seems unlikely.
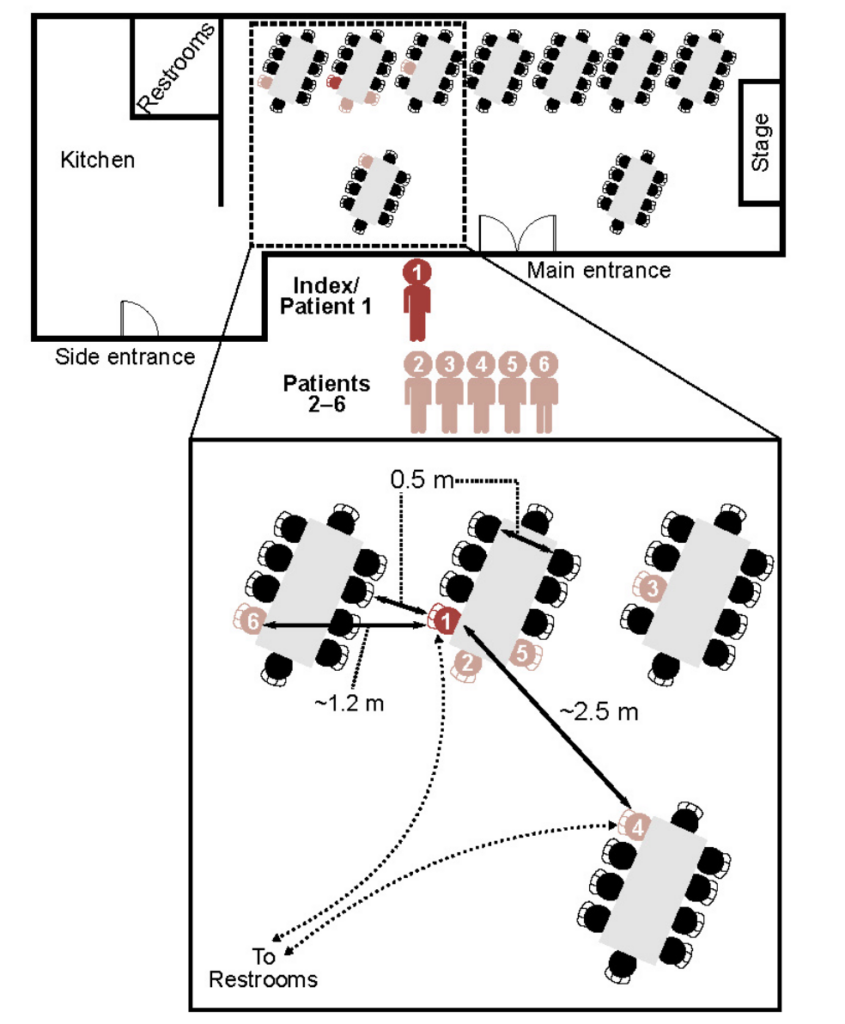
This paper (2025-12-02) reports on an outbreak in Argentina of 2018/2019 Andes Hantavirus (ANDV) which started at a birthday party. There are things that say you should worry and things that say you should not.
Worrisome things:
- The index patient was only at the party for about 90 minutes, and there were about 100 people at the party.
- The diagram of the seating chart showed that three people were seated at different tables.
- One of the three seated at a different table, Patient 4, crossed paths with the index case on the way to/from the bathroom, but they just said hello — there was no physical contact.
- The paper said that “the route of infection in secondary cases was possibly through inhalation of droplets or aerosolized virions”, i.e. that ANDV spreads through the air.
- The paper said that Patient 2 “was the most likely source for six infections in other persons during the early prodromal phase”. (“Prodromal” means “in the early symptoms stage”.)
- Three people (two patients and one hospital administrator) caught ANDV in the hospital. The two patients who caught it there both shared rooms with people who had ANDV.
Reassuring things:
- Approximately 95% of the guests at the birthday party did not get sick. Even 70% of the people who were at the same table as the index case did not get sick. The person sitting to the index case’s left didn’t even get sick.
- Zero of the health care workers who attended any of the patients got sick, and not many of them were wearing PPE.
- The paper did not uncover any transmissions while infected people were asymptomatic. (That doesn’t prove that there was absolutely zero asymptomatic spread — contact tracing is not 100% accurate — but it does suggest that asymptomatic spread is not a major driver of transmission.)
- There is very short period between “starting to feel sick” and “trouble breathing, go to hospital (or die)”. This, coupled with above, limits how many people a sick person can infect. 😐
- This post (2026-05-10) reports that ANDV doesn’t mutate very fast: there is very high degree of similarity between the MV Hondius outbreak’s variant and the ANDV outbreaks in Argentina in 1997 and 2018.
- This review paper (2021-09-13) on human-to-human transmission of ANDV finds fault with previous papers, complaining that they didn’t do a good enough job of checking to see if there were rodents around the infected people and that the contact tracing relied on people’s (falible) memories. (Me, I think they are insisting on a standard of proof that is higher than is appropriate for our purposes.)
- In the paper about the 2018 outbreak, the R0 dropped significantly when mitigation measures restricting human movements were put in place. If humans only caught it from rodents, restricting human activities shouldn’t have caused such a sharp drop.
- This US CDC report (2018-10-19) says that a woman sick with ANDV took two flights inside the US, and none of the 53 contacts they traced got Andes. (And there wasn’t an epidemic, so it doesn’t look like they just missed tracing somebody.)
- This US CDC report (2003-09) about Argentina reports that in an area of northern Argentina, there were about 30 reported cases of hantavirus, with most cases being mild and a mortality rate of 13.7%. Furthermore, they found antibodies in 6.5% of the population — which suggests that its actual mortality rate is even lower than 13.7%. (NB: tests don’t do a good job of distinguishing between ANDV and the Sin Nombre hantavirus (SNV) of the US Southwest — which does not spread human-to-human. I couldn’t find information about whether Argentinian rodents carry SNV.)
- This paper (1998-12) from Argentina looked at the prevalence of ANDV antibodies in healthcare workers at the hospital where most patients in a 1997 outbreak. They found that the prevalence of ANDV antibodies in the healthcare workers was about the same as in the community — meaning they probably were exposed by rodents and not by patients. (The paper mentioned that the healthcare workers didn’t always wear gloves and never wore facemasks.)
- Hantaviruses have been around for a very long time — hundreds if not thousands of years — and there has not been a hantavirus pandemic (that we know of).
- Unlike COVID-19 in 2020, we know how to diagnose and test for hantavirus already. (We humans still aren’t very good at treatment yet: right now the best we humans can do is treat the symptoms: give patients breathing tubes, put them on dialysis when their kidneys shut down, put them on ECMO when their lungs shut down, etc. But at least we humans know what to watch for.)
Note that “it spreads through the air” and “it’s not very contagious” can both be true, and are scary/reassuring for different populations. “it spreads through the air” is scary for individuals (because you never know if you are going to be one of the susceptible ones), but “it’s not very contagious” is reassuring for populations (because it’s not going to go wildly out of control).
In this interview (2026-05-14), an esteemed epidemiologist points out that in a cold-weather cruise like MV Hondius, you’re going to need to push around a lot of warm air to keep people warm, so that changes how much people are exchanging air, so it doesn’t need to be close contact. (Editor: There’s a lot of air pushed around in office buildings, too!) He also points a number of cases where there was no spread, and thinks that we’ll see a small number of superspreaders and essentially nothing from anybody else; he predicts that this will all be over in two or three weeks. (Editor: unless someone caught it on the last day on the ship, and the virus incubates for 42 days…)
This paper (2007-06-01) from Argentina reports that they found ANDV virus in the blood of patients 5 to 15 days before they developed symptoms. I hope they are testing the blood of everybody who was on the MV Hondius!
Recommended Media
This article (2026-05-13) does an excellent job of explaining why politicos and public health people are making hantavirus sound more benign than it is, but why you still shouldn’t worry about hantavirus… but you should still worry about the fractured state of health care systems are around the world.
In this video (2026-05-10) and this article (2026-05-12), a doctor explains that hantavirus spreads through the air. One of his pieces of evidence is a conversation he had with a doctor on the MV Hondius (the passenger who stepped in, not the ship’s doctor who got sick and was evacuated).
This post (2025-05-12) gives a background on hantavirus, a little bit about epidemiology of the MV Hondius outbreak, and then about halfway down goes into why we do not have reason to panic.
In this video (2026-05-11), a doctor describes what a case of hantavirus pulmonary syndrome (HPS) looks like medically, and then goes a little bit into why he doesn’t think members of the public should worry.
RSV
Immunization
💉 This paper from France (2026-05-07) reports that maternal vaccination (with RSVpreF) and post-birth nirsevimab similarly effective if the RSVpreF was given at least eight weeks before delivery. Otherwise, nirsevimab was better:
| time before birth | nirsevimab advantage |
| 6-8 weeks | +20% |
| 4-6 weeks | +20% |
| 2-4 weeks | +55% |
Apparently, it takes time for Mom to manufacture and deliver antibodies.
Measles
Transmission
According to the Government of Canada Measles and Rubella Monitoring Report (updated 2026-05-12), in the week ending 2 May 2025, the following jurisdictions had the following number of new measles cases:
- Canada: 45;
- Manitoba: 32;
- Alberta: 5;
- BC: 4;
- Quebec: 3;
- Ontario: 1.