Vaccine clinics
I have now seen three different clinics in action: Creekside Community Centre when I escorted a friend of mine, Costco yesterday when I escorted my husband, and today at the independent Davie Pharmacy for when I got mine. (Yay!)
The three clinics spent radically different amounts of time with each patient:
- At the Creekside Community Centre with elderly clients who phoned in, they spent a LONG time going over the information with the patients.
- At Costco, where Favourite Person had booked online and filled out form online, they spent close to zero time talking with him. They basically handed him a form and that was it.
- At Davie Pharmacy, an independent, the vaccinator took his time with me and made very sure to go through the explanations carefully, repeatedly asking if I had any more questions. Probably less time than at Creekside, but way more than Costco. I also had answered “yes” to one of the questions but did not volunteer that, as a test to see if he noticed & would ask me about it — and he did.
The three locations also had very different vaccination cards. Creekside didn’t offer my friend a card. At the pharmacies, they gave us things whose printing, coloration, etc. looked identical to their prescription forms (which the Davie Pharmacy owner confirmed). He also carefully told me how to get at the electronic record.
I asked how I got a form for a “vaccine passport” and he said that “they” were still trying to figure out what those would look like. So I think for now, our vaccine records will need to live on our phones.
I did not see the lot information on the prescription, nor the manufacturer (although the Costco one did have the manufacturer). I assume those are in the electronic record, it’s something that clearly is very important to Dr. Henry.
Press Briefing
This was a very dense briefing.
VOC proportion
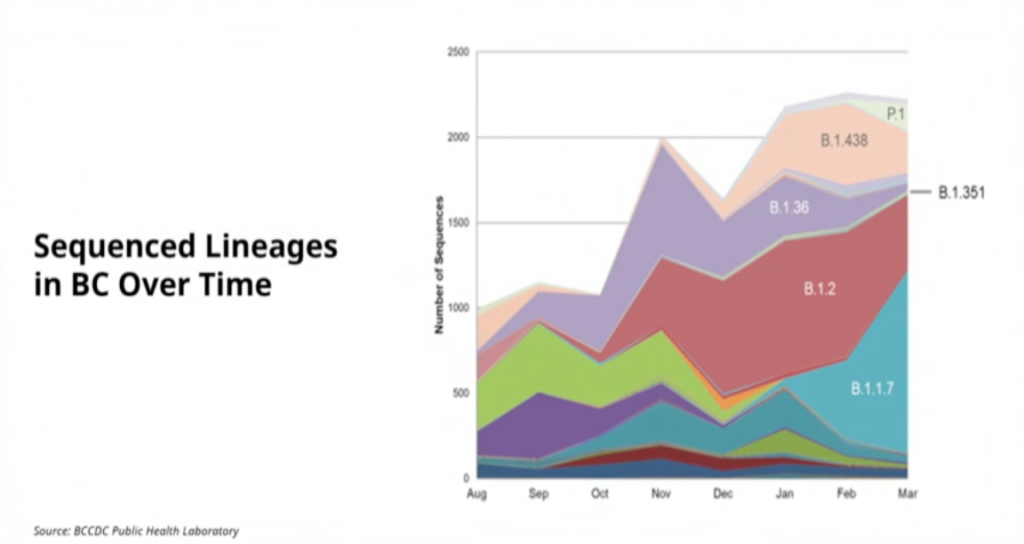
Dr. H showed a slide of the number of cases by each variant over time. I thought the most interesting thing was how it didn’t lead me to any obvious conclusions. Note: the B.2, B.1.36, and B.1.438 variants are one which are not particularly scary. Well, no more scary than COVID classic.
VOC sequencing
Dr. Henry spent a lot of time justifying a change in VOC surveillance/reporting. Instead of doing (fast) SNP screening on (almost) all the positives and then doing whole genome sequencing on all the ones which SNP said were suspicious, they are going to still do SNP on almost all the positives, but do random sampling on the rest.
She never actually said, “we can use our resources better” or “we’re getting too many cases to sequence all of them”, but I suspect that’s the bottom line. Instead, she said things like, “we don’t need to sequence them all to know that we’ve got VOC in the province, we know we have VOC”.
Somehow this will allow them to focus their whole-genome sequencing capacity on understanding new transmission chains, determining the proportion of travellers who have VOCs, and monitoring for reinfections, vaccine failures, and escape variants.
If you don’t understand how only doing a sampling will make that easier, well, I don’t either.
P.1
Dr. H mentioned that the P.1 rates look high because we actually test a lot for P.1 — more than in all of the US.
It looks like P.1 hits younger people in part because there happened to be P.1 clusters in Whistler which spread among that young cohort. The amount of P.1 is still small in a relative context — around 6% right now — so I think we should expect to see older people get P.1 as time goes on.
One thing she mentioned was that the P.1 samples show up more easily than the other strains. I guess that means that there are fewer false negatives with the P.1 than the other strains?
Hospitalizations
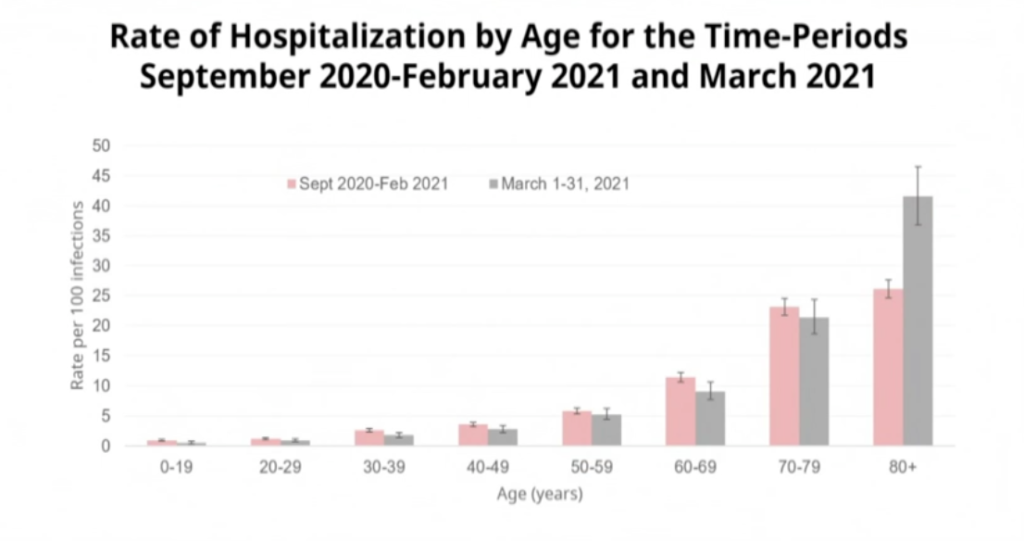
Dr. H showed a slide of the hospitalizations by age. She said that they’ve been seeing more young people in hospital, but that in general, that appears to be just because more people are going to hospital.
There has been a slight increase recently across kind of all age groups, except that the 80+ rate has dropped a lot (yay vaccines!). Note that the graph is confusing: the pink bars are newer and the grey is older, despite pink being to the left of the grey.
They are seeing more hospitalizations from P.1. Note that young people are overrepresented because P.1 was mostly at Whistler, among young adults at first.
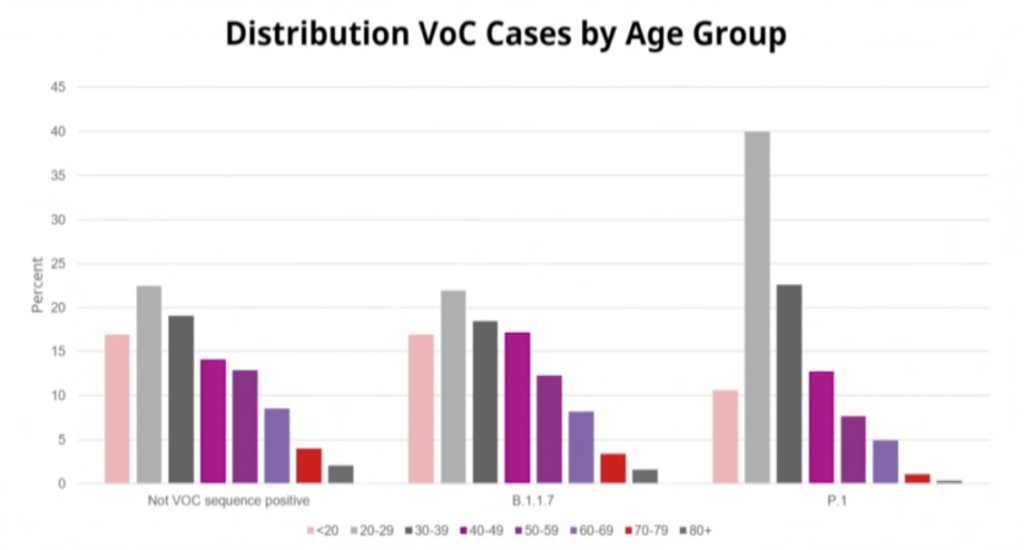
There is not much increase of B.1.1.7 over non-VOC (note that the error bars overlap) tho there is a bit of a diff in the 50-69 age group. There is a bit of a difference for P.1. P.1 has small numbers of people, so not clear if the difference is real.
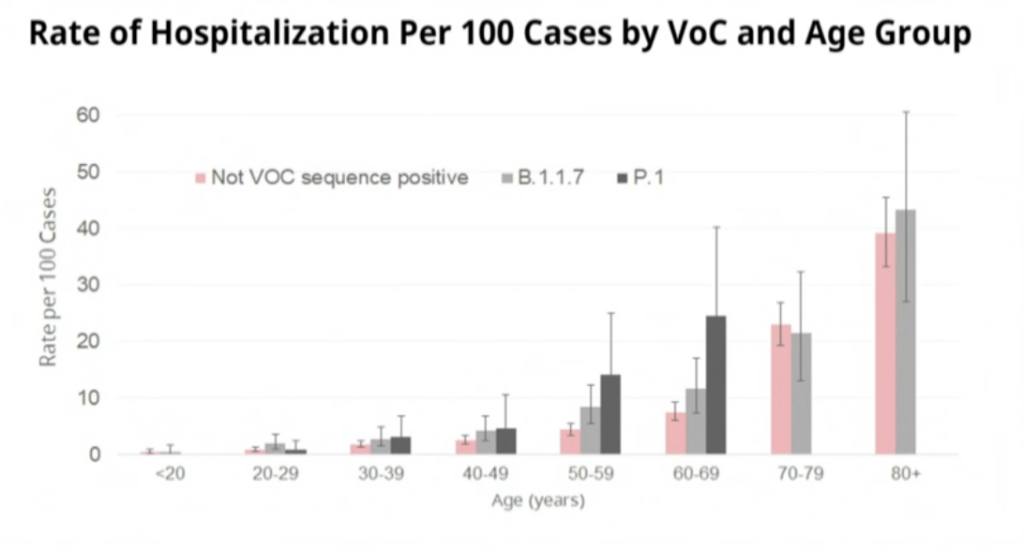
Vaccinations are great, but it looks like you have to get above some threshold before you really see a difference:

Measures
Dr. Henry put in a new Order today, to take place on Monday. Basically, if three people get sick at a non-essential workplace, WorkSafeBC officials can shut it down immediately for up to ten days.
(Me: “You mean they didn’t have that power before??”)
She said that this would allow BC to be more surgical in its closures, instead of using the blunt instrument of sector closures.
Survey
Dr.H announced a second survey, similar to the one that 400K of us did in the fall.
Tone
Dr.H had a slightly different emotional tone. Yesterday, she visited Surrey Hospital, and every time she talked about the visit, she choked up a little bit. It wasn’t like the waterworks turned on, she never had to stop, but it clearly affected her.
She also was… a bit more pissed off? She was always polite, she didn’t storm and rage — only men are allowed to display that much emotion — but I had the sense that she was frustrated with the irresponsible people who were flouting the rules. She couldn’t say that, but that was the sense I got. It was subtle, but I’ve watched a lot of these briefings.
This was the first briefing I have ever seen where she did not close with some variation of “be kind, be calm, be safe”.
Vaccines
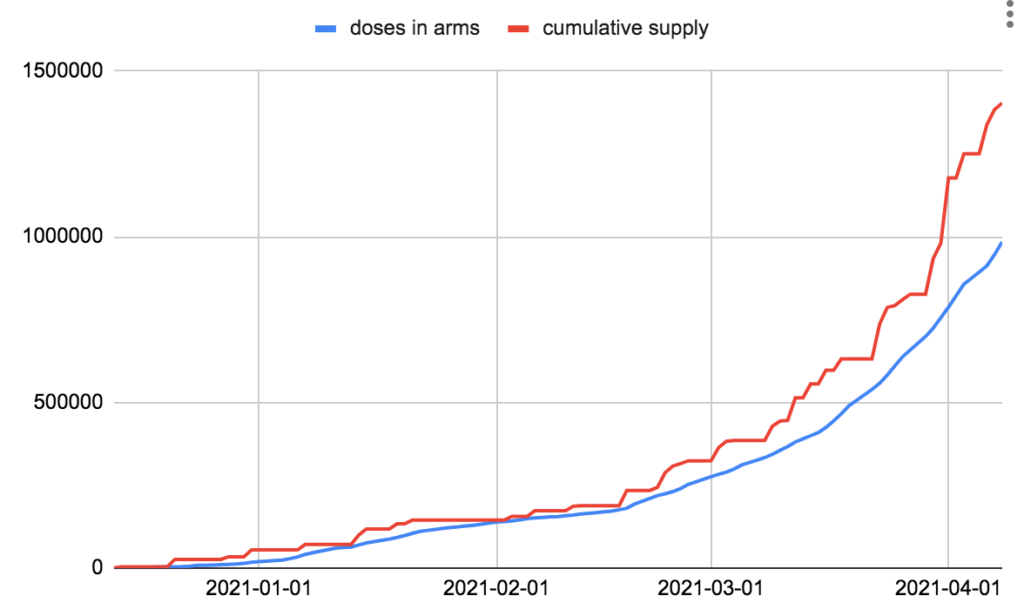
Dix addressed people who have been bitching about how we have too much vax in the fridges and not enough in people’s arms. He basically said, “look, we never know when the vax is going to arrive, it’s hard to make plans when we don’t know”. He said that we’ve vaccinated about 20% of the people who are eligible.
He said that BC has the capacity to go through (essentially) as much vax as they will give us.
Health Care Capacity
Minister Dix talked about health care capacity, and gave a ton of statistics. He said we have 730 ventilators, and we have a bunch more in reserve. At the moment, about 146 ventilators (20%) are occupied at the moment, 40 by people with COVID.
Q&A
Note: these are heavily, HEAVILY and snarkily paraphrased.
Q: Why aren’t we vaccinating first responders faster? A: Because AZ got shut down for people under 55. We are diverting some of the mRNA to places where we see especially high risk. (I saw some discussion somewhere — maybe in the briefing? maybe Twitter? that part of why the first responders weren’t getting diverted mRNA was because they didn’t actually have a lot of cases in their ranks.) We will be ramping up the occupation-based track as soon as we get more vax, like the J&J which we expect to, hope to, get in a few weeks, and when the feds let us use the AZ.
Q: The positivity rate for schoolkids is a whopping 10-14%, wtf, how can you say there is minimal transmission in schools??? A: Check the dates: those tests were done when the kids were coming BACK to school after Spring Break. The number of cases in the schools is going to go up as levels in the community go up, that’s not a surprise. So if ANYONE in the household is sick, ALL Y’ALL best be getting tested ASAP and isolate yerselves. ESPECIALLY IF Y’ALL WERE NAUGHTY OVER BREAK by travelling or socializing.
Q: With the change in sequencing strategy, what data are you going to publish how and when? A: Uh, we’re working on figuring that out.
Q: How long does it take to distribute the vax? A: Dix: Rant rant rant the manufacturers don’t deliver when they say they will rant rant rant, normally about a week from when it gets to the BC distribution centre to when it gets to the clinics. Usually 2-3 days, though sometimes it takes longer to get to our rural clinics. We have a lot of capacity, an over-capacity, in delivery.
Q: Are you concerned about capacity in Metro Van hospitals? A: Of course, especially since hospitalizations are a lagging indicator. We’re going to see an increase for the next while. The staff is dealing, but it’s a concern. Note, one problem we’ve been having is people delaying treatment because they are scared of hospitals, so they don’t come in until they are really sick. DON’T DO THIS. Our hospitals are safe, our ERs are safe, so see your doc, call 911, go to the hospital, do what you need to do. Dix: It’s fair to say that while overall utilization is low, there’s pressure in Metro Van. DrH: We are looking at how we can shift people around, like we did for Prince George when UNBC had that awful outbreak.
Q: There was a video of twenty people partying on a houseboat, what rules do houseboats fall under? A: They fall under the same rules we put in place in last summer and which haven’t gone away: there are limits on rentals, with fines for the organizers of parties, the people who rent to them, and the attendees, and the police will enforce this. DO NOT DO THIS!
Q: Dix: Why do we only have 70% utilization? I interpreted the question about ventilators, but Dix answered as if it was about vaccine usage. A: Rant rant rant suppliers rant rant you can’t distribute vax before you receive it.
Q: Should people line up to try to get doses which would otherwise go to waste? A: NO! We have processes in place to make sure we don’t waste doses. We call people on the wait list, we take doses to the emergency room, etc. We don’t throw doses away, please don’t line up.
Q: Some people say we should shift to giving doses to young people who spread, what do you say? A: The people going to hospitals and going on vents are still older people, so we’re sticking to older-first, and continuing to do outbreak response. And don’t underestimate what we have already done: we have already vaxxed a shitton of the people in the riskiest jobs: food processing, farms, a bunch of people at Whistler.
Q: Why did the Measures have to be changed? A: They’re not changed as much as evolved. We wanted to be more precise.
Statistics
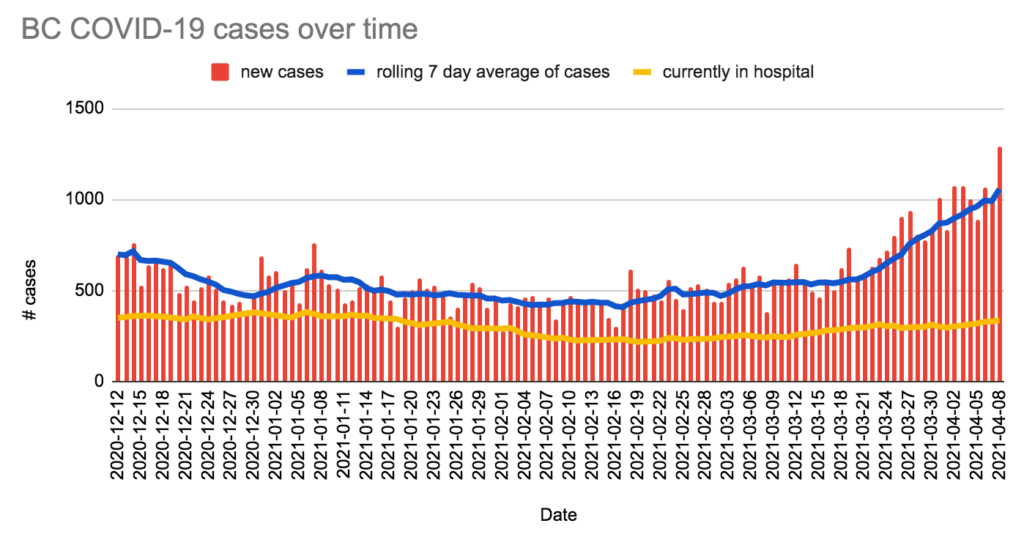
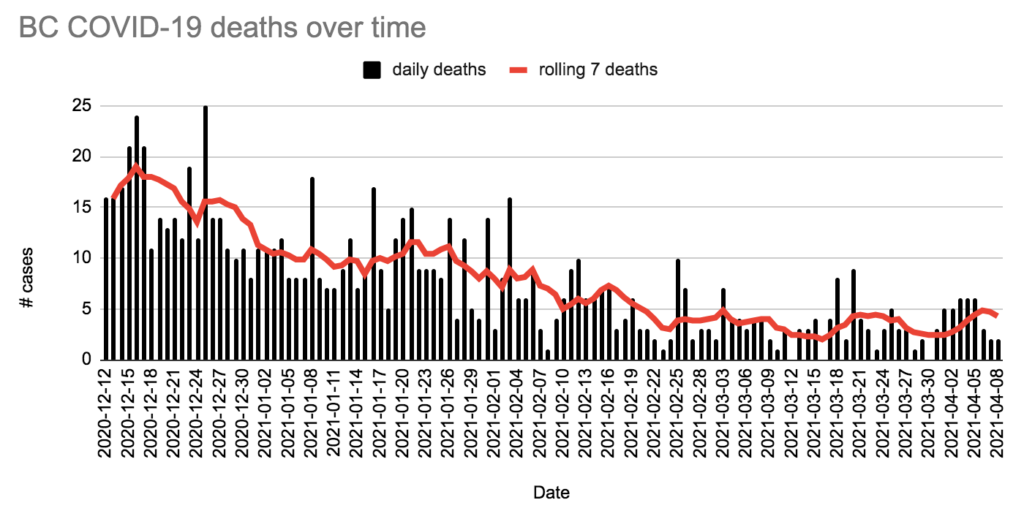
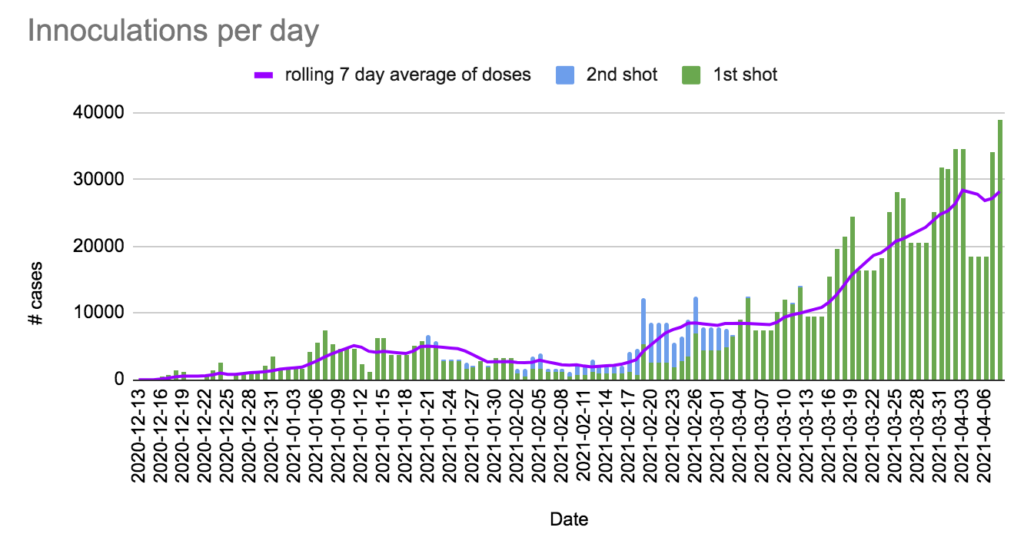
+1,293 cases, +2 deaths, +38,905 first doses, +60 second doses, +8813 AZ doses.
Currently 336 in hospital / 101 in ICU, 9,184 active cases,15,203 under monitoring, 97,462 recovered.
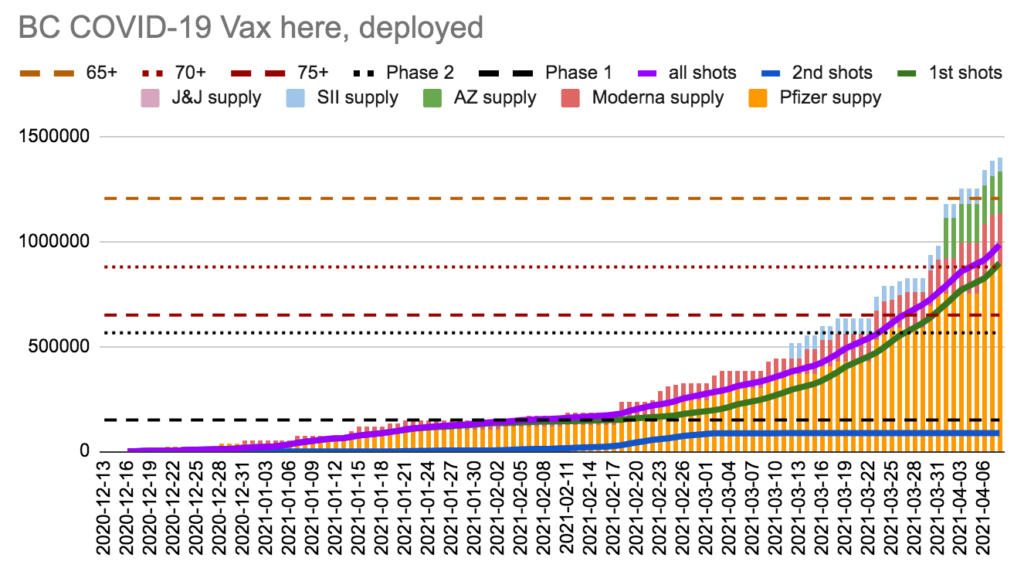
We have 418,509 doses in the fridge; it will take us 10.75 days to use it at today’s vax rate. We have injected more doses than we had received by 8 days ago.
Charts