
Long COVID
I was puzzled for a long time: all the statistics I saw said that Long COVID was really common — from 5% to 50%, depending on which study you looked at — but I didn’t know anybody with Long COVID! How could this be? I thought maybe it was because my echo chamber is largely affluent, but that didn’t seem to make sense.
This tweet made me realize that it’s not that I don’t know anyone with Long COVID, it’s that I don’t know that I know anyone with Long COVID. There are lots of reasons why people might not talk about it:
- Fear of discrimination, especially fear of losing a job.
- Not wanting people to focus exclusively on the illness; not wanting their identity to be subsumed as “that person with Long COVID”.
- Not wanting to listen (again!) to how COVID and/or Long COVID doesn’t exist.
- Not wanting to listen (again!) to pet theories about how to fix it (take iron! meditate! essential oils! take up jogging! hydroclorizine!).
- Embarrassed to admit that they failed to take adequate precautions to keep themselves from catching it.
- It’s none of anyone’s damn business.
- Their version is a much milder case than it could be, and they don’t want their friends to freak out.
- For COVID minimizers, not wanting the embarrassment of having to admit that COVID-19 was in fact a big deal.
- Not even knowing that Long COVID is a thing.
I am embarrassed to admit that those didn’t occur to me even though I myself have a medical condition which I do/did not routinely disclose for reasons 1-4 (even though #1 doesn’t much apply any more).
Addendum: I added #3, #4, and #5 after this was published.
This recent tweet thread (and this older tweet thread) have nice reviews of recent (and older) research on Long COVID. This thread focuses specifically on papers looking at vaccination and Long COVID.
I believe I have covered all of the research either in the past or in this blog post, but if you want it all in one place (well, okay, three places), here ya go.
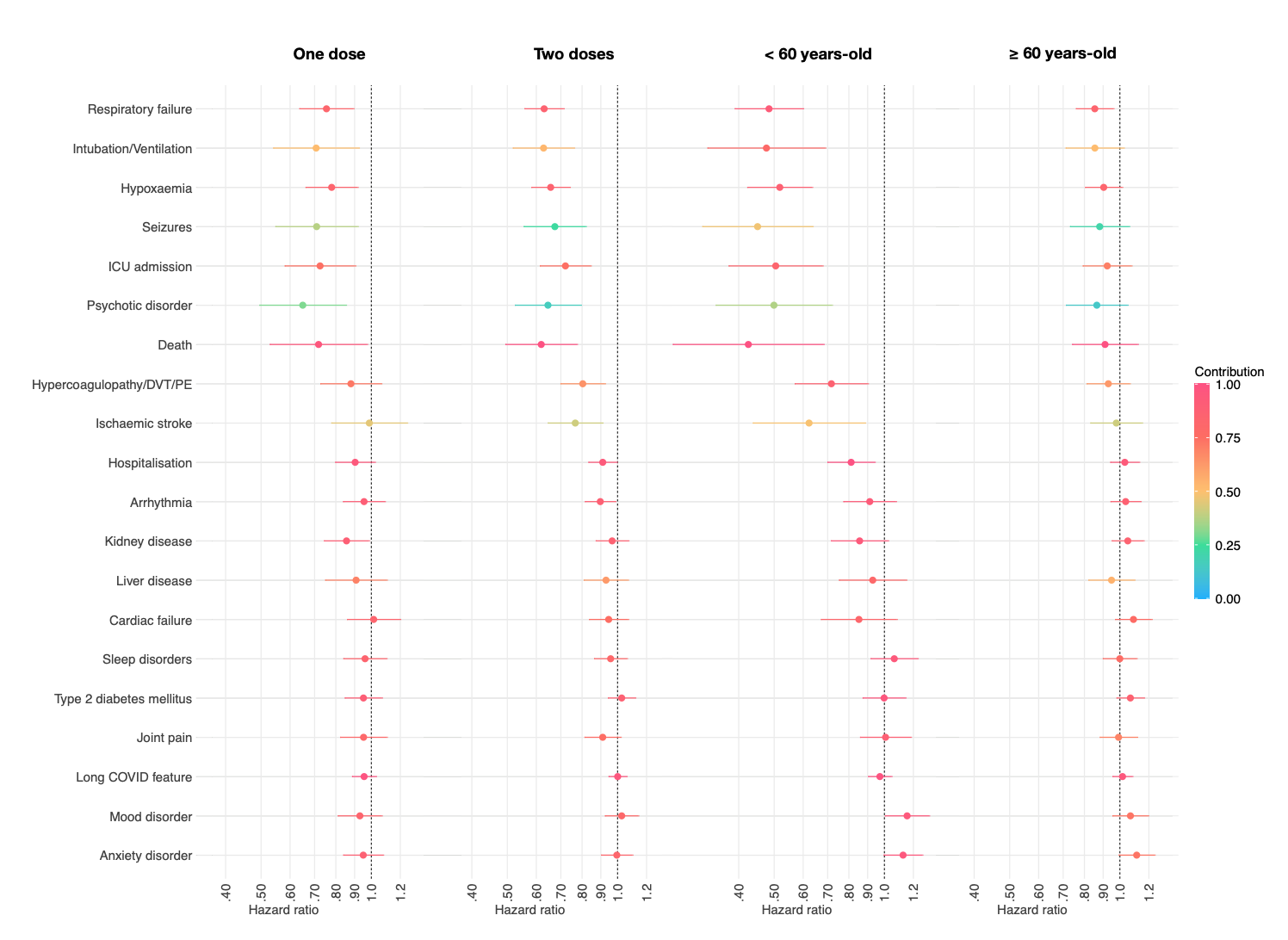
This paper out of the UK found during Feb-Sept 2021 that people with one dose of vaccine were 12.8% less likely to develop Long COVID than those with zero. People with two doses were an additional 8.8% less likely to get Long COVID than those with zero doses.
This paper from the USA (from November) looked at specific symptoms, and found a small benefit (~10% at best) of vaccination against many Long COVID symptoms. (NB: I don’t really like this paper because it focuses on ummm medical symptoms like “heart disease” and not what I think are more common but more subjective things like “brain fog”.
This study from Israel (in Jan 2022) found that people who had two doses of vax (which in Israel would be mRNA) had lower risks of various Long COVID symptoms:
- fatigure: 64% less likely;
- headache: 54% less likely;
- weakness: 57% less likely;
- persistent muscle pain: 68% less likely.
This preprint from Indonesia (from Jan 2022) says that people who have two shots of a viral vector vaccine have 31% lower risk of their sense of smell getting f’ed up.
I try to limit what I say about other countries, but OMG this governmental report says that 3.1% of the entire UK population (NOT just people who had COVID-19, the entire UK population!) self-reports as having Long COVID.
Vaccines
This article reports that Health Canada just approved boosters for 16- and 17-year-olds.
This article reports that Pfizer has submitted its application for toddlervax to the US FDA. The US FDA will probably approve it in mid-June; Health Canada usually approves in roughly the same timeframe.
This preprint says that high-risk patients who got an injection of Evusheld were only 34% as likely to get a COVID-19 infection, 13% as likely to get hospitalized, and 36% as likely to die (all-cause mortality). (Yes, I know Evusheld is not actually a vaccine, but it is used like one.)
Mitigation Measures
This preprint from the USA surveyed people on how often they wore a mask and if they got COVID-19 infections. (NB: I think the survey was overweighted to health care workers.) People who did not always wear a mask were more likely to catch COVID-19 than those who always masked, but it varied by variant period:
- not-always were 66% more likely to get infected in the pre-Delta period;
- 53% more likely in the Delta period;
- 16% more likely in the Omicron period.
I’m not sure what to make of that. One way to look at it is “f* it, masking doesn’t help all that much now, why bother”. Another way to look at it is “clearly cloth masks were good enough for pre-Delta but aren’t any more, I’m going to always wear N95s”. (The study did not ask about cloth vs. N95s masks.)
This paper found that people who reported doing more social distancing got COVID-19 less often:
- 42% less likely for those who always distanced with people they did not know;
- 64% less likely for those who always distanced with people they knew;
- 60% less likely for those who sometimes distanced with people they knew.
Variants
This preprint says that BA.4/BA.5 are worse than BA.1, BA.2, on pretty much all measures. This preprint says that BA.4/5 are more evasive.
It isn’t a huge that BA.4/BA.5 are nastier, but I think I never actually said so. (Wait, you thought it was A Rule of Nature that viruses always got milder? No, no, it is not. That’s only true when the disease is so nasty that at first it kills its hosts off before they can transmit it. With COVID-19, which can spread before there are symptoms, there is no evolutionary pressure on it to become milder.)
BTW, you were wondering why BA.4 and BA.5 are always mentioned in the same breath? Because they have the same spike proteins. The differences between them are in non-spike areas of their DNA.
This preprint says that the time to PCR “conversion” (which I think means time from positive test to negative PCR test) is about the same for Delta and Omicron, with a median time of six days.
Treatment
This preprint out of Hong Kong during the BA.2.2 wave says that Paxlovid reduced mortality by 75% and hospitalization by 31%. It reduced something which I think translates to “needing critical care in hospital” by 53%.
Rates were similar across ages and vaxxed/unvaxxed status. Molnupiravir didn’t work as well, reducing mortality by 39% and not reducing the risk of hospitalization. It did reduce what I think means “critical care” by 36%.
This preprint from Israel says that patients over 65 on Paxlovid were only 33% as likely to be hospitalized and 19% as likely to die. It didn’t work as well for people ages 40-64: patients on Paxlovid were 78% as likely to be hospitalized and — if I understand this right — 64% more likely to die. (Note, however, there was a small sample size of the 40-64 year-olds; check out the huge confidence interval on the second graph.)


This paper from the USA found that pulse oximeters significantly overestimated the oxygen saturation of people with dark skin, and that led to significant undertreatment of Black and Latino patients.
Transmission
This preprint out of German says that there is NO COVID-19 present in breath you exhale if you are just breathing normally (no talking, yelling, singing, sneezing, coughing, or exercising). This is pretty extraordinary if true. (Caution: it was a small sample size.)
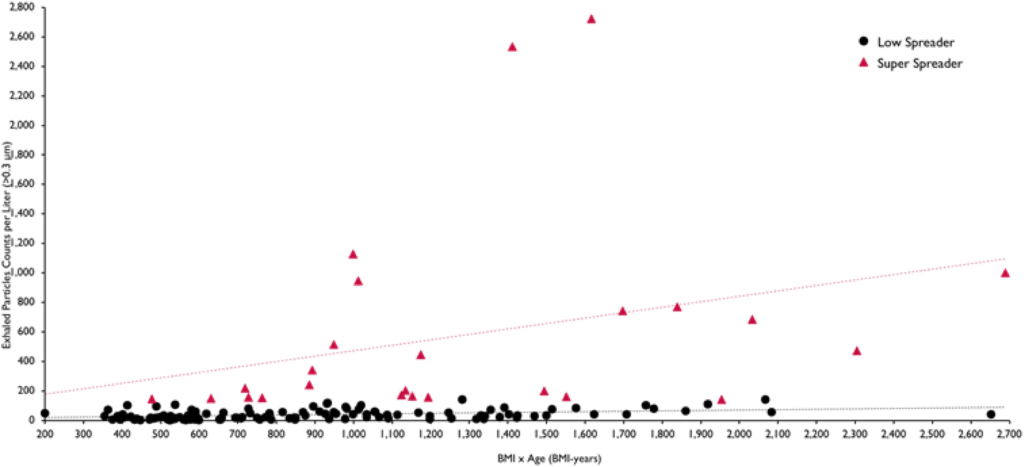
I found this old paper (from Feb 2021) which said that the amount of aerosols produced went up with severity of obesity and age in humans (and degree of COVID-19 infection in monkeys), and that 18% of the subjects accounted for 80% of the aerosols.

Testing
This preprint found that in New York City (which has good testing infrastructure), cases were undercounted by 30X. Thirty. Three-zero.
While BC is not New York City, I see no reason why we would be magically better.
This paper from France says that they trained dogs to smell COVID-19, and they did really really well. (This is consistent with this paper I mentioned before from Finland.) The dogs were 97% accurate, with a specificity of 91% (true negative rate) and sensitivity of 90% (true positive rate). Dogs had especially good specificity (94%) and sensitivity (100%) for asymptomatic individuals. (Antigen tests, for comparison, have specificity of 84% and sensitivity of 97%.)
Recommended Reading
If you are worried about a kid under five, you can read this blog post to get a very detailed discussion of all the vaccines for under-5 year-olds.
This article warns that COVID-19 is not a one-time deal, people are going to get it over and over again (unless we get better vaccines).
This post is a how-to guide for vaccinating hard-to-reach communities.