
Folks, we have a problem.
We have a problem with language. When I say “Long COVID”, you probably immediately think “brain fog and/or fatigue” (and maybe you’ll think of a persistent cough and/or loss of smell/taste). What you probably do not think of is a higher chance of severe illness/death from something that doesn’t look like COVID-19: diabetes, heart attacks, etc.
But there’s something else, perhaps more import, going on with post-COVID stuff: the risk of dying in the next year — from any cause — is about twice as high for people who have had COVID-19 than from people who have not. (And it might go on longer than a year — the only studies which I have read have stopped after a year.)
What if this risk stays with you? Or even if the risk only lasts for a year and then stops (though that seems unlikely), what if every time you get COVID-19, the clock starts again? (That seems likely, as a big study of US military veterans found that people with two COVID-19 infections had double the risk of all-cause mortality as people with one infection.) With COVID-19 being endemic, if you don’t pay attention, you probably will get COVID-19 every year. If your risk of all-cause death doubles, I think that means that your expected years of life got cut in half. That’s a lot of years! I’m ~60, and I rather expect to live to ~80. That would mean that COVID-19 might take ten years off of my life.
(I have noticed that I don’t talk about this issue much with my friends who have had COVID-19 infections, in part because it feels kind of rude to tell people that can’t do anything about it that they are likely to have a shorter lifespan. 🙁 That might be part of why we don’t talk about this.)
We don’t have a catch-all name for the long-term side effects of COVID-19, which makes it hard to talk about. Long-Term COVID Side Effects? Long Damage? Excess Morbidity/Mortality? (People don’t know that “morbidity” means sickness, so that’s not great.) Friends of COVID? COVID-Related Years of Life Lost?
The best term I’ve come up with is COVID-Related Excess Death and Sickness, which has the nice feature of having a nice acronym (CREDS). If you have a better term, please let me know. I am going to start putting CREDS under a separate heading.
There will be some overlap between Long COVID and CREDS, for example, papers which explore damage to cells by COVID-19. I’ll put things that relate to both under Long COVID, and I’ll try to put the Long COVID and CREDs sections next to each other.
Long COVID
This preprint from USA confirmed that Paxlovid does decrease the risk of getting Long COVID, by like 25-30%, comparable to the 26% that an earlier study found.
Some good news! This paper from UK reports that patients with fatigue-primary Long COVID had significantly less mental and physical fatigue after four weeks of a drug which helps mitochondira, AXA1125.
COVID-Related Excess Deaths and Sickness
This paper from Taiwan using US data found that the risks of autoimmune disorders was way way higher in the six months after getting COVID:
| Disease | Adjusted Hazard Ratio |
| rheumatoid arthritis | 2.98 |
| ankylosing spondylitis | 3.21 |
| systemic lupus erythematosus | 2.99 |
| dermatopolymyositis | 1.96 |
| systemic sclerosis | 2.58 |
| Sjögren’s syndrome | 2.62 |
| mixed connective tissue disease | 3.14 |
| Behçet’s disease | 2.32 |
| polymyalgia rheumatica | 2.90 |
| vasculitis | 1.96 |
| psoriasis | 2.91 |
| inflammatory bowel disease | 1.78 |
| celiac disease | 2.68 |
| type 1 diabetes mellitus | 2.68 |
| death | 1.20 |
This paper from UBC (go UBC!) found that people in BC who tested positive COVID-19 tests in the first two years of the pandemic were 17% more likely to get diabetes than people who had not. For males, it was even worse — a 22% higher risk. This meant about 3.4% of the new diabetes cases in BC resulted from COVID-19 (4.75% for males).

The risks got higher as the COVID-19 infections got worse: 142% higher risk for those hospitalized and 229% higher risk for those admitted to the ICU.
This blog post talks about the UBC paper and another TWELVE studies which also found increased risk of diabetes after COVID-19 infections, plus talked about possible mechanisms.
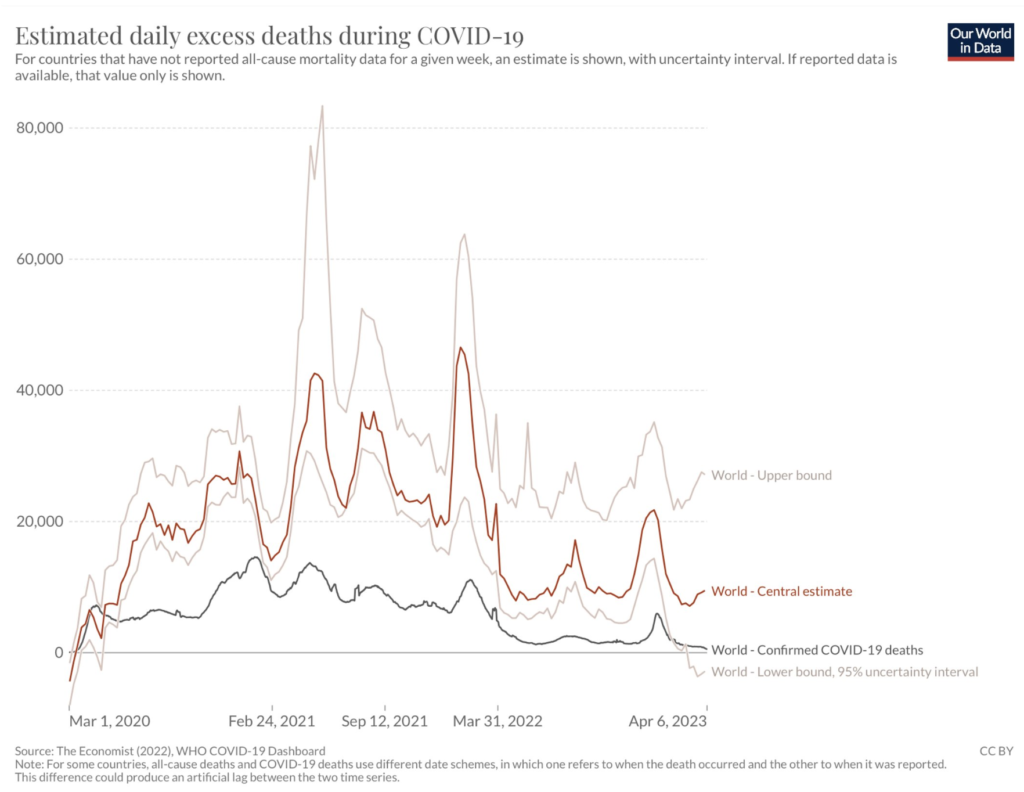
As per this tweet (referring to the graph below), the global COVID-19 death rate is going down, but the excess deaths are going up. How can this be? It’s a sign that COVID-19 causes long-term damage to the human body, which manifests itself in early deaths that don’t look like COVID-19.
This paper from the US found that hospitalized COVID-19 patients were much more likely to get secondary infections in the hospital (e.g. catheter-associated urinary tract infection) than non-COVID-19 patients. They don’t know if it’s just from the longer hospitalization stay (8.2 days for COVID-19 patients vs. 4.7 days for non-COVID patients), maybe it’s due to COVID-19 wards being more frantic, or if it is from something about COVID-19 itself.
This paper from USA found that baby boys born to mothers who had COVID-19 infections during pregnancy had twice the risk of a diagnosis of a neurodevelopmental issue than mothers who did not have COVID-19. Baby girls were not affected.
This paper from UK found that 62% of people who had been hospitalized with COVID-19 had sleep disturbances after they got out, and that having sleep disturbances correlated with having impaired lung functioning. Yeah, I also can’t sleep well when I can’t breathe well (from a stuffed up nose). (Oddly, the study authors framed it the other way around, as if trouble sleeping caused trouble breathing.)
Mitigation Measures
This report from the USA (from 27 Feb) says that COVID-19 deaths from 1 June to 31 December 2020 have a negative correlation with mask mandates:

Vaccines
This article reports that the US is launching a USD$5B program to develop better vaccines and treatments for coronaviruses (not just COVID-19, but also common cold coronaviruses, SARS, and maybe even MERS).
This paper from Hong Kong reports that a nasally-administered live attenuated influenza vaccine, DelNS1-RBD4N-DAF, is more effective than the mRNAs in mice and hamsters. Nasal vaccines are coming, y’all! (I just don’t know when. Two years, maybe?)
Interestingly, they use a modified influenza virus as the vector for depositing the spike-instructions payload, and they found that this one vaccine gives some immunity to influenza as well, meaning it has real potential to be a combo flu/COVID vax!
This paper from Pfizer says that they get better results in hamsters when they give two doses of regular Pfizer (BNT162b2) and one of a new vax (BNT162b4) which targets non-spike SARS-CoV-2 proteins (which change less from variant to variant). Pfizer has started Phase 1 trials in people.
One downside of using non-spike proteins is that it might make it more difficult to tell if someone has been infected or not. (Right now, it’s easy to tell because there are antibodies to the nucleotide in people who have been infected and not in people who have never been infected.)
This article reports that a bunch of vaccines in Canada are going to expire this year: 16.8M out of 18.5M.
This shouldn’t be a surprise to anybody: Canada way overbought as a way to guarantee that we’d get some. My old page of vaccine contracts — which I think was from before the vaccines even shipped — shows that the minimum contracted was enough for like 95M people to be “fully vaccinated”.
This paper from the USA found that vaccination didn’t affect length of menstruation, but about 4% of the participants found they had a higher quantity of bleeding.
This large study from the USA found that the rate of venous thromboembolism (VTE) from vaccines was 0.1% over the baseline rate. (By contrast, it says VTE happens in 8% of patients hospitalized with COVID-19 and 22.7% of COVID-19 patients admitted to the ICU.)
Transmission
This paper from Australia found that school contract tracing programs, masks, testing, and vaccination, and public information campaigns help reduce the spread of COVID-19, while school closures did not have a significant association with the prevention of COVID-19 infection in educational settings.
This paper from Netherlands found that intellectually disabled adults were about five times more likely to die from COVID-19 than the general population..
Treatments
This preprint from USA says they’ve found two monoclonal antibodies, 12-16 and 12-19, which works really well against every variant they’ve tested against. They say it works by jamming the spike into the stuck-closed position. (The spike is normally closed, but has to open up to “get into the cell.”open the lock” to get into the host’s cell.)
This paper from USA also reports finding a new, broadly effective monoclonal antibody, S728-1157. They mention that this antibody is more effective when the spike is in the “closed” position.
This paper from Brazil found that people who tested positive for COVID-19 who were given oral fluvoxamine (a very cheap, widely available anti-depressant) plus inhaled budesonide (a corticosteroid) were hospitalized at about half the rate of ones who were given a placebo.
Pathology
This paper from USA found that not only does SARS-CoV-2 block major histocompatibility complex class I expression (which is a technical way of saying that SARS-CoV-2 keeps cells from calling for help from T-cells), but Omicron is even better at blocking the cries for help than other strains.
This means that it’s difficult for the body’s T-cells to clear out infected cells, which suggests that the infection can persist for a long time. (And indeed, autopsies keep finding SARS-CoV-2 reservoirs all over the place, including the brain and the testicles.)
This paper found that, across 142 countries, the higher percentage of obese people in the country, the higher their COVID-19 mortality rate.
This paper from Netherlands found that patients with cognitive impairments declined faster during facilities lockdowns than they did in non-lockdown situations. Interestingly, people with dementia did not decline as fast as people with mild cognitive impairment or subjective cognitive decline.
Recommended Reading
This article gives a lay overview of Long COVID.
This article talks about “how did no-mitigation measures-Sweden have such a mediocre pandemic?” tl;dr: Vaccination matters way more than mitigation measures, its mitigation measures ended up being pretty middle-of-the-road, in part because the important thing is what people actually do and not what the policies are.
This article talks about temporary but scary changes in menstruation after COVID-19 vaccinations, and how hard it was to make The Establishment take them seriously.
This article has a great headline: “Why aren’t we hearing about COVID waves anymore? Because COVID is at ‘a high tide’ — and staying there”.

This article is about Long COVID: how it’s still here and how it’s worse than you think.