
Health news was harder to find this week. A lot of my sources were overrun with articles about what trouble the new US president is fomenting, leaving little room for articles about COVID, mpox, or H5N1. ☹️
You might have noticed that I sometimes mark snippets with “AGAIN”. Why do I bother showing studies that show what we already know? Sometimes there are areas where different studies show different things, and I tag snippets with “AGAIN” in part to emphasize that this is not one of those areas — that different studies show again and again that this is something we already know.
COVID-19
Long COVID
This paper from Germany (2025-01-23) reports on Long COVID.
- 61.2% of people with Long COVID had never smoked, compared to 75.7% of fully recovered patients;
- 30.2% of people with Long COVID were obese, compared to 12.4% of fully recovered patients;
- 38.7% of people with Long COVID had qualified for university, compared to 61.5% of fully recovered patients;
- 35.6% of the people with Long COVID had post-exertional malaise;
- 11.6% of the people with Long COVID had symptoms consistent with ME/CFS.
This paper from USA (2025-01-21) reports that children of different races have slightly different symptom prevalences. For example, Latinx kids had hair loss more frequently, Black kids had fewer skin symptoms, and Asian/Pacific Islanders had more POTS than White kids.
AGAIN This paper from USA (2025-01-22) reports that women get Long COVID more than men, with interesting subgroup analyses. Compared to men:
- 🤯 women in the 18 to 39 age group only had a 4% higher risk;
- overall, women had a 44% higher risk when only adjusted for only age, race, and ethnicity;
- women had a 31% higher risk when adjusted for only age, race, and ethnicity and also demographic, clinical, and social determinants of health;
- non-pregnant women had a 50% higher risk;
- women 40-54 y/o had a 42% higher risk if they were menopausal and a 45% higher risk if they were non-menopausal.
🎉 This paper from Italy (2025-01-24) reports that they have found a set of eight chemokines which are higher in kids with Long COVID. They used the study’s data to train an AI model and can predict if a kid has Long COVID with an accuracy of 93%!
Transmission
😬 This paper from Germany (2025-01-23) found that almost all children in their study had evidence of a COVID-19 infection, even though a significant number said they’d never had COVID-19. 93.3% had antibodies to the nucleocapsid protein (which you don’t get from vaccination), but only 67.9% said they had had a COVID-19 infection — meaning 25% had had a COVID-19 infection and didn’t know it.
The study also found:
- 7% of the respondents had Long COVID symptoms for more than three months;
- Vaccinated kids had 12% fewer acute flu-like infections than unvaxxed kids;
Treatments
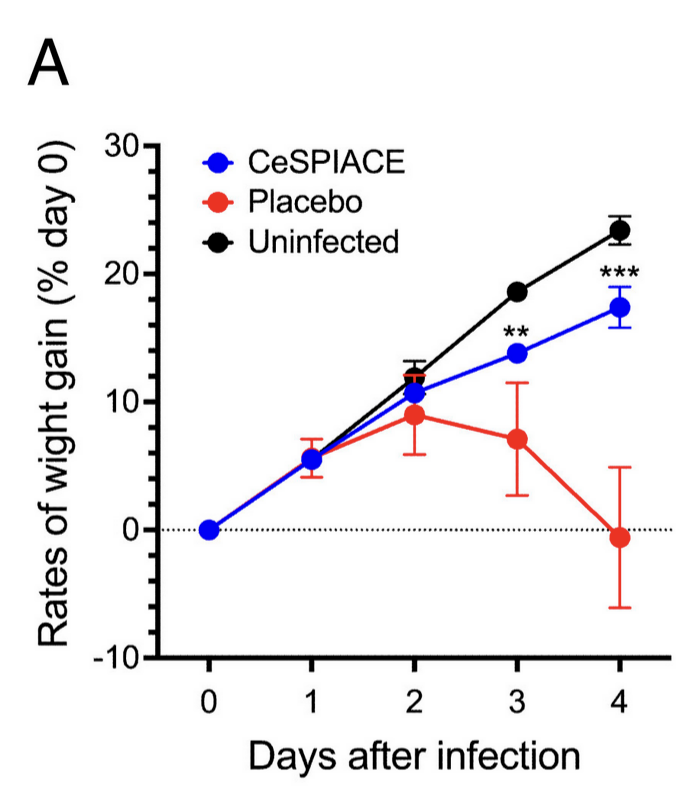
🎉 🎉🎉 This paper from Japan (2025-01-24) reports that the authors designed and made a peptide (a short chain of amino acids) which blocks the COVID-19 spike very effectively across multiple different variants. They also say that it should have minimal side effects and be very cheap to produce.
They gave hamsters the peptide an hour after the COVID-19 dose, then once per day for three days, and the hamsters barely noticed a high dose of Delta while the placebo hamsters all died (and quickly). 🙁
It’s not clear to me: if this got approved, would it be mostly used a prophylactic, a “morning-after” treatment, or a treatment once symptoms occurred?
🎉 This older article from Australia (2023-07-17) (non-paywalled version) talks about a person who uses nasal heparin every day and has not gotten COVID-19. I don’t see why heparin would work, and it’s a small sample size (n=1), but this is another example of “putting stuff in the nose works much better against COVID-19 than it really ought to”.
AGAIN This paper from USA (2025-01-17) reports that Paxlovid works well against COVID-19. They found that Paxlovid given within five days of diagnosis:
- reduces the risk of hospitalization by 39%;
- reduces the risk of death by 61%;
- reduced the risks more for people over 65 than for younger people;
- dropped the risk about equally for both vaccinated and unvaccinated patients.
Pathology
❓ This paper from Jordan (2025-01-23) reports that spike proteins of various coronaviruses (including two common cold coronaviruses, some bat viruses, Gamma, Delta, and COVID Classic) might make prion misfolding easier, based on some computer modelling of their structures. The paper also said something about mRNA vaccines possibly also being a problem, which I saw some people being concerned that this meant that they should avoid mRNA vaccines and get Novavax instead.
Looking at the paper more carefully, it’s not the mRNA vaccines themselves that are the (potential) problem, it’s the spike protein. It doesn’t matter where the spike protein comes from: dumped in like Novavax, made by your cells by the mRNA or by SARS-CoV-2, if the spikes are bad, all of them are bad. And as a practical matter, you are going to get spikes, you just have to choose where you get them from: vaccines or COVID-19?
(Thanks to @datum@zeroes.ca working through this question with me!)
Also, it’s not entirely clear how much spikes, SARS-CoV-2, and the mRNA vax can cross the blood-brain barrier (BBB). If something doesn’t cross the BBB, it cannot make prions in the brain.
SARS-CoV-2 absolutely crosses the BBB, like this paper (2024-03-09) gives rock-solid evidence for, saying it goes through the olfactory bulb. Papers like this one (2024-02-22) report that COVID-19 infections kill endothelial cells, which in turn make the BBB “leakier”.
I have not seen as much about vaccine spikes making it into the brain, but a quick search finds that vax spikes absolutely sometimes do. This assessment report (2021-03-11) of the Moderna Classic vax by the European Medicines Agency said that they did find mRNA in the brains of vaccinated rats but at very low levels, “(2-4% of the plasma level)” which I think means 2-4% of the level it was at in the bloodstream. Is that too much? I don’t know.
Should we be concerned about nasal mRNA vaccines, given that SARS-CoV-2 enters via the olfactory bulb? I don’t think so. A nasal mRNA vax could hijack cells in the olfactory bulb to make spikes, but then those spikes don’t hijack other cells; the mRNA hijacking doesn’t have a way to climb from the olfactory bulb to the brain.
Should we be concerned with nasal self-amplifying RNA (saRNA) vaccines? Um. Maybe. SaRNA vaccines do make more of themselves, so maybe they could traverse the neuron between the olfactory bulb and the brain? I’m sorry, I don’t know enough about saRNAs. In particular, I don’t know what makes saRNAs stop. It might be that saRNAs break down after the third cycle, and that’s not enough cycles enough to get to the brain. Sorry.
What would (I think) reduce this possible, theoretical problem is vaccines that are made up of just an important piece of the spike, like this paper (2024-10-21) and this paper (2023-08-01) describe.
Note that it’s not just COVID-19 spike-protein vaccines that could have this (potential) problem: any molecule could have this problem, and they even identify two “common cold” viruses that score high on “relative probability of there being a problem”.
I also don’t know if certain configurations of proteins can, in fact, promote prions, or if the technique the paper uses can find those configurations. (Sorry, I chose to allocate time to other COVID articles instead of chasing a whole new subject matter area.)
Recommended Reading
Want to feel really good about BC’s vaccine rollout? Read this (long, old) article (2022-12-09) about the USA’s vaccine distribution clusterfuck 💀. Among the things I learned was that storing vax was not actually a big deal — Pfizer’s vax keeps for ten weeks at fridge temperature!
This report (2023-08-29) discusses why Sweden’s pandemic response was relatively successful. Tl;dr: they actually did have some restrictions, and people voluntarily did things they were advised to do, instead of the government forcing them. In the end, they had a similar number of deaths as their neighbours and significantly lower than the USA and UK. Also, their neighbours with harsher lockdowns delayed COVID-19 deaths, they didn’t avoid the deaths. This blog post (2025-01-20) has a slightly more critical analysis.
H5N1
Transmission
This article (2025-01-21) says that H5N1 is still spreading in the US. Poultry outbreaks continue (but they have been going on for years, so I don’t really feel like they are news), six more housecats in five states have died, and another infected dairy herd in California was detected. The US national total of ever-infected dairy herds is now 930 and California’s is 713.
🐦⬛💩 In this article (2025-01-25), an infectious disease specialist speculates that bird flu could spread in windblown poo dust. This is speculation, but um yuck and oh-fuck.
Vaccines
This paper from China (2025-01-22) reports that poultry flocks vaccinated against H5N1 do not get infected with H5N1 as often as unvaccinated flocks 🎉, but also cautions that the virus mutates faster in areas where flocks are vaccinated 😞.
Marburg
Oh great. This press release (2025-01-20) reports that Tanzania has a confirmed Marburg case.