
Long COVID
This paper from UK (2024-02-07) found that the REGAIN intervention — an eight-week rehab program — helped people with Long COVID more than the usual care (one 30 min session). The REGAIN intervention had roughly one hour per week of light physical exercise and one hour per week most (six) weeks of psychotherapy, all given in small groups via Zoom.

COVID-Related Excess Deaths and Sickness
This paper from Japan (2024-02-07) found that elderly patients who had been hospitalized with COVID pneumonia and bacterial pneumonia had more functional decline after one year than people who only were hospitalized with COVID pneumonia. They also noted that co-infection with bacterial pneumonia was more common with Omicron than with previous variants.
This paper from Vietnam (2024-02-04) found that three-quarters on people who had had a COVID-19 infection that did not require hospitalization said they had insomnia after the infection. 22% said that the insomnia was severe.
This paper from USA (2024-02-02) found that people who had COVID-19 infections spent 178% of their baseline healthcare on healthcare in the year after a COVID-19 infection, even given that 94% of the people in the study had not been hospitalized. The cohort that was not hospitalized for COVID-19 had a 103.5% increase in the number of outpatient visits, a 33.7% increase in ER visits, a 300% increase in the number of inpatient visits, and a 403% increase in the number of days spent in hospital. It was worse for the hospitalized, for example, the cohort which was hospitalized had a 1700.0% increase — 17 times as many — in the number of days spent in hospital.
Overall, after a COVID-19 infection, people had
- A 166% increase in the number of blood disorders;
- a 123% increase in the number of endocrine and metabolic disorders;
- a 115% increase in nervous system disorders;
- a 76% increase in digestive system disorders;
- a 75% increase in mental and behavioral disorders.
This paper from USA (2024-02-09) found that veterans who had recovered from COVID-19 infections used healthcare at a much higher rate in the year after their infection than baseline. It fell significantly over the course of a year, but was still slightly elevated at the end of the year compared to controls.
The number of excess visits was higher for those over 80 than those 20 to 40 years old, but not as much as I would have thought (6.1 visits per month vs. 4.8 visits per month). There was also a slight difference in vaccinated vs. unvaccinated excess visits (4.5 visits per month vs. 3.2 visits per month).
Vaccines
This paper from USA (2024-02-06) found that the BA.4/5 bivalent vaccine was 49.4% effective in kids against symptomatic COVID-19 and 54.0% effective against lab-confirmed COVID-19, compared to kids who had never been vaccinated or had only been vaccinated with monovalent vax.
This paper from USA (2024-02-16) found that getting the first two doses of Pfizer in different arms gave a much better IgG antibody response and neutralizing titres than getting both vaxes in the same arm. The difference was slight at first (1.1x), but rose to 1.4x by 14 months later.
This contradicts previous papers which found that same-arm Pfizer was better, like this one paper from Germany (2023-08-11) and this one from Israel (2022-11-30). One might suspect that the difference is that the studies were small, and the German one was smaller (n=303) than the new USA one (n=947), but the Israeli one was huge (n=2,678,226). The difference might be follow-up time: the German study looked at IgG levels after two weeks; the Israeli study looked at how many people got infections in the next 38 days.
(This older paper from UK (2015-01-07) found that opposite-arm rabies vaccinations worked better (n=509), and this older paper from UK (n=303) found that babies who got Tdap, polio, influenza, and PCV13 in opposite-limbs had better tetanus IgG responses than same-limb babies, but immunity levels were similar for other pathogens.)
This paper from Sweden (2024-02-06) found when mothers were vaccinated when pregnant, the vaccine absolutely did not hurt their babies. Their babies had a 32% lower risk of death from all causes, 22% lower risk of neonatal nontraumatic intracranial hemorrhage, and 27% lower risk of hypoxic-ischemic encephalopathy.
Pathology
This paper from Australia (2024-02-09) found that COVID-19 promoted microbiological changes in the placenta which are associated with hypoxia and placental dysfunction.
This paper from USA (2024-02-08) estimated that how susceptible you are to COVID-19 is 57% genetic and 34% the environment (mostly where you live/who you live with, I think). This did change over time: genetics were less important than environment before about October 2020. (Because vaccines weren’t available yet, I am going to guess it had something to do with variants.)
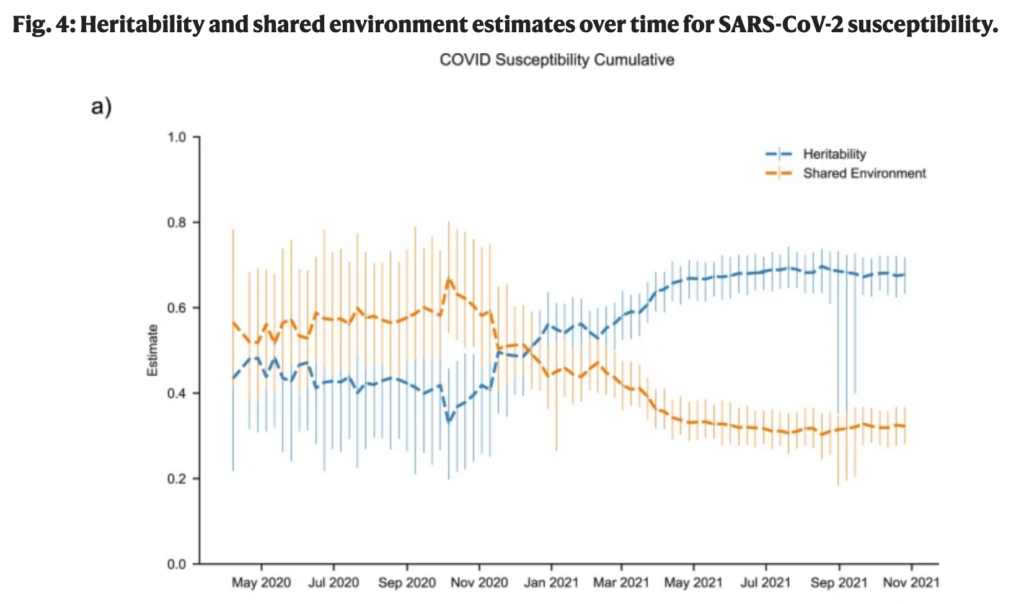
They, alas, don’t know what in the genes affects your susceptibility per se, although this paper found that people with type O blood were 30% less susceptible than those with A or B blood; this paper found that people with O (especially) and A were less susceptible than those with A or B type and that almost all of the COVID-19 patients were Rh+ (98%, vs. ~85% in Canada). (This preprint, however, said that people with type O blood were about four times more likely to get Long COVID.)
Transmission
This Mastodon thread points out a few things that I knew on one level, but it brought them to the forefront. She points out that 1918 had far less favorable conditions for the virus:
- There are a lot more people in the world now — 8 billion vs. 1.8 billion. Every person that COVID-19 infects is a laboratory which gives the virus an opportunity to mutate, so there are ~4.4 times as many opportunities to mutate and make more dangerous viruses.
- In 1918, our medical treatments were not good enough to keep immunocompromised people alive, like they are now. Research has shown that SARS-CoV-2 can mutate pretty much indefinitely inside an infected immunocompromised person.
- In 1918, we didn’t have routine intercontinental air travel (or even good roads!). COVID-19 can travel much more easily now.
- In 1918, our buildings were much leakier, which meant ventilation was better — especially in the summer. Without air conditioning, all the windows were generally wide open in the summers.
- In 1918, we didn’t try to defeat the Spanish Flu with medicine which deliberately mutated the virus, unlike now with molnupiravir.
Testing
This paper from USA (2024-02-01) found that the excess deaths due to sickness that were not coded as COVID-19 deaths in the USA were correlated well with COVID cases. In other words, a significant fraction of excess deaths coded as non-COVID were, in fact, due to COVID-19. The authors estimated that 162,886 excess deaths were due to COVID but not counted as such — 13% of the number counted as COVID-19 deaths!