
Long COVID
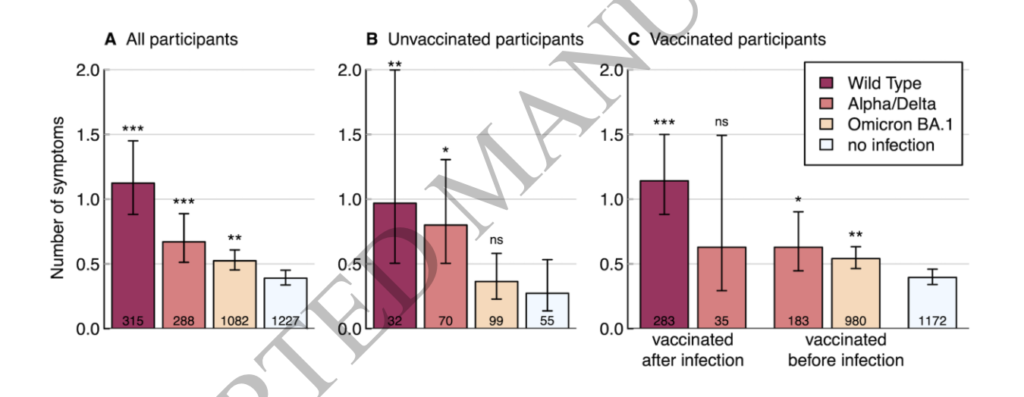
This paper from Switzerland says that there are fewer Long COVID symptoms after an Omicron infection than for previous variants. The number of symptoms on a survey given to people who tested postive were:
| Strain of infection | # Symptoms |
| COVID Classic | 1.12 |
| Alpha/Delta | 0.67 |
| Omicron | 0.52 |
| no infection | 0.39 |
Interestingly, for Omicron infections, getting vaccinated didn’t reduce the risk of Long COVID!
This presentation from Switzerland reports that health care workers were 67% more likely to get Long COVID after COVID Classic than from Omicron in 2022Q1, but only 37% more likely to get Long COVID after COVID Classic than Omicron in 2022Q3. So Omicron was not as bad, but Q3 Omicron was worse than Q1 Omicron?
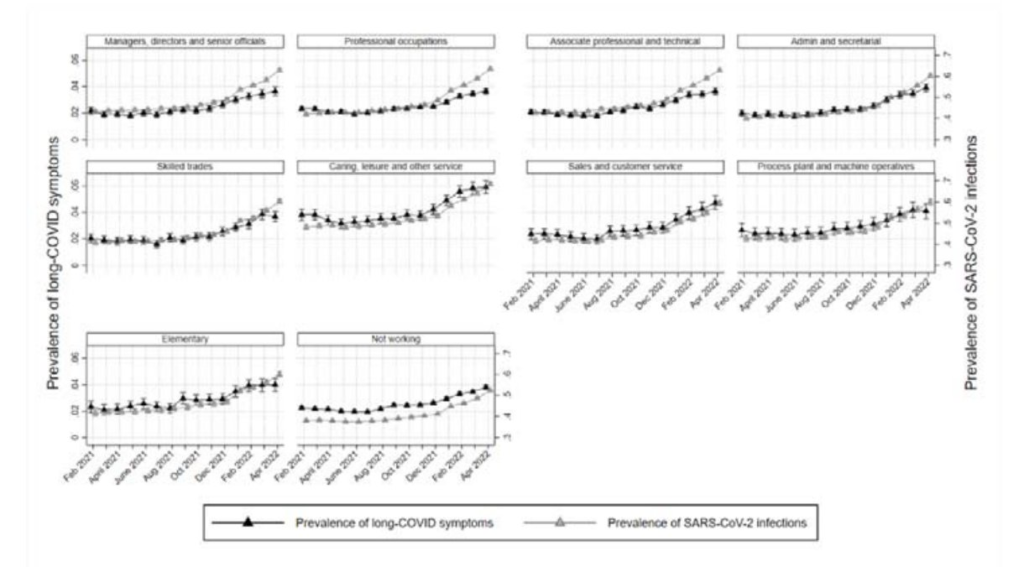
Wow this is strange: different occupations have different rates of getting Long COVID and of how severe it is for them. In general, the higher your profession’s risk for COVID-19, the higher the risk for Long COVID. This did not hold for professional and technical careers.
As far as really severe symptoms, the probability of reporting Long COVID symptoms varied a lot by industry:
- Financial services: 7.7%;
- teaching and education: ~22%;
- unemployed: 27%
Pathology
This report from the US found that people who had been hospitalized for COVID-19 had visible changes in their eyes compared to people who had COVID-19 but were not hospitalized and those who had not had COVID-19. People who had been hospitalized had 8% lower densities of retinal capilaries and had decreased volume of some areas of the eye.
Unintended Consequences
Using data from FitBit, this paper from the USA says that people logged ~700 fewer steps per day during the pandemic than before.
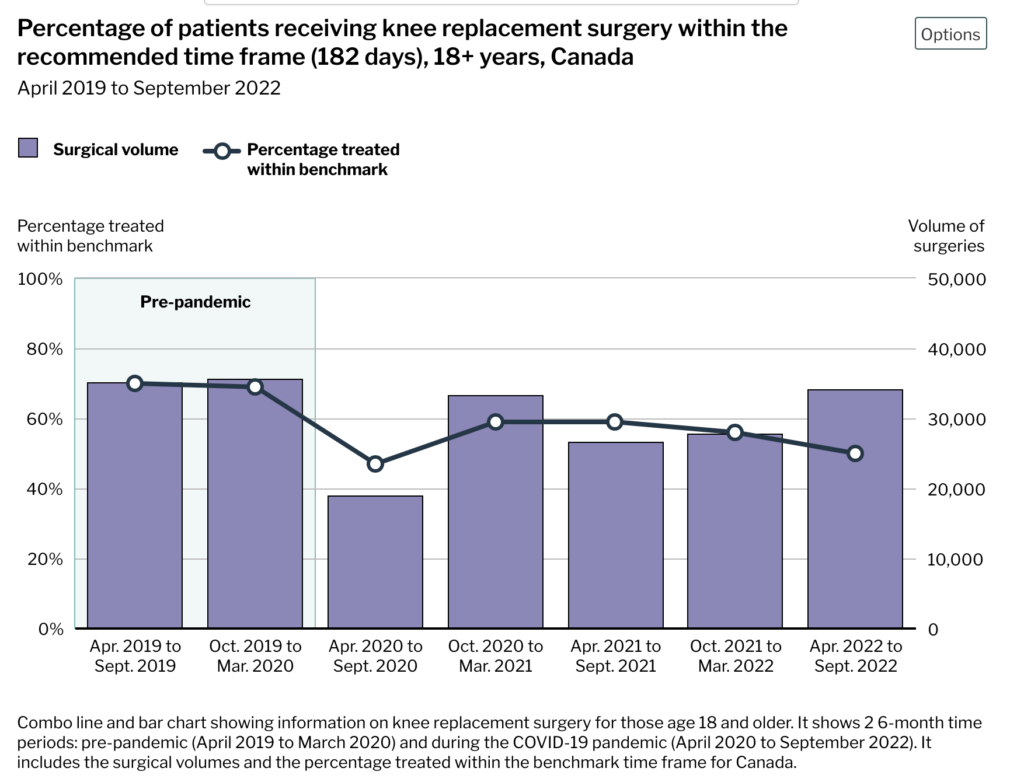
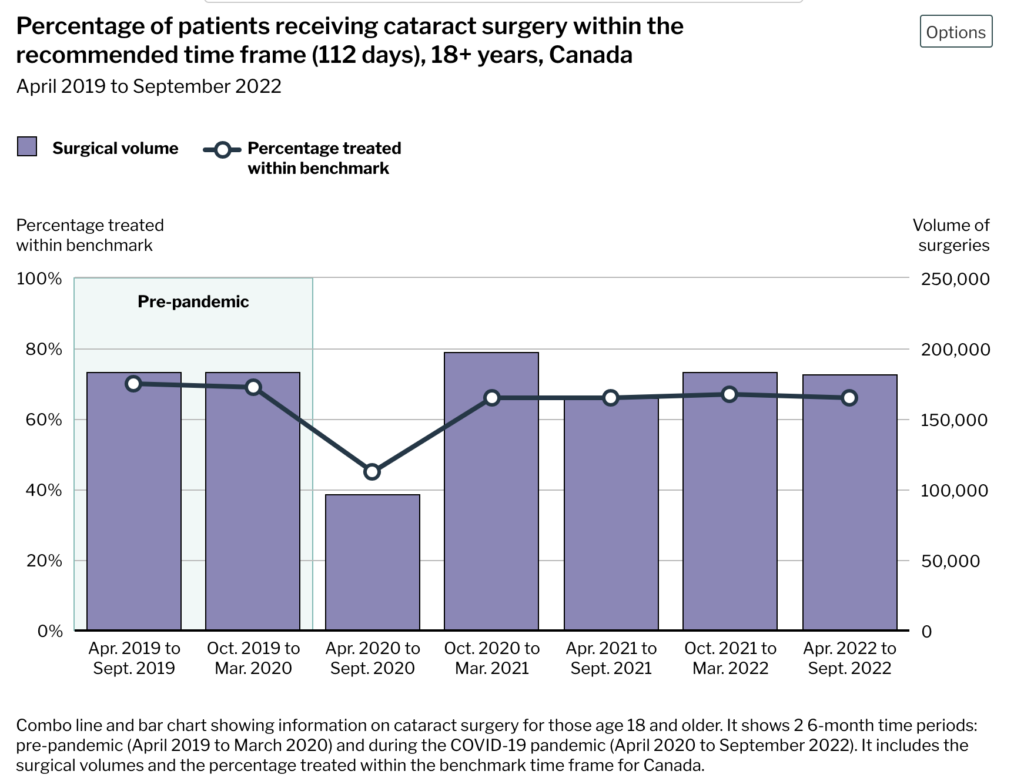
This report says that knee replacement and cataract surgeries were the surgeries most delayed in Canada by the pandemic. Cancer surgeries were also slightly delayed, but generally only a few days. This might have been in part because a lot fewer cancers got diagnosed (because people were avoiding health-care settings).
The report pointed out that knee replacements haven’t caught back up as fast as cataracts because knee replacements require operating rooms, while cataract surgery can happen in outpatient clinics.
Pathology
This article (reporting on this paper from Sweden) says that blood from children who were not exposed to SARS-CoV-19 sometimes had antibodies which reacted to SARS-CoV-19, and the presence of those antibodies correlated strongly with antibodies to OC43 — one of the “common cold” coronaviruses.
This article from India says that, anecdotally, patients are reporting urinary tract infections as a side effect of COVID-19.
This paper from UK found that the people who were in the highest 20% of DHA (an Omega-3 fatty acid) had a 21% lower chance of catching COVID-19 and a 26% lower chance of getting hospitalized than those in the bottom 20% of DHA.
This paper from the USA reports that mothers who get COVID-19 while they are pregnant have a higher risk of obesity.
Vaccines
This preprint from USA reports that they got very good results (as tested in the blood of macaque monkeys) with a vaccine made from the spikes of four different strains: COVID Classic, Alpha, Beta, and Gamma. Importantly, they saw a good immune response against Omicron, despite not having any Omicron strains in the mix.
This press release says that the European Medicines Agency (who approves/rejects vaccines for the EU) approved Bimervax as a booster today. Bimervax is made of proteins which — near as I can tell — make up a kind of Frankenspike with pieces of the Alpha spike and pieces of the Beta spike. Interestingly, HIPRA, its parent company, started out in Spain making vaccines for animals in 1971. I believe that Bimervax is their first human vax.
Transmission
This paper from Finland says that their proprietary protein nasal spray was able to protect mice from COVID-19 completely when administered eight hours ahead or four hours after exposure.
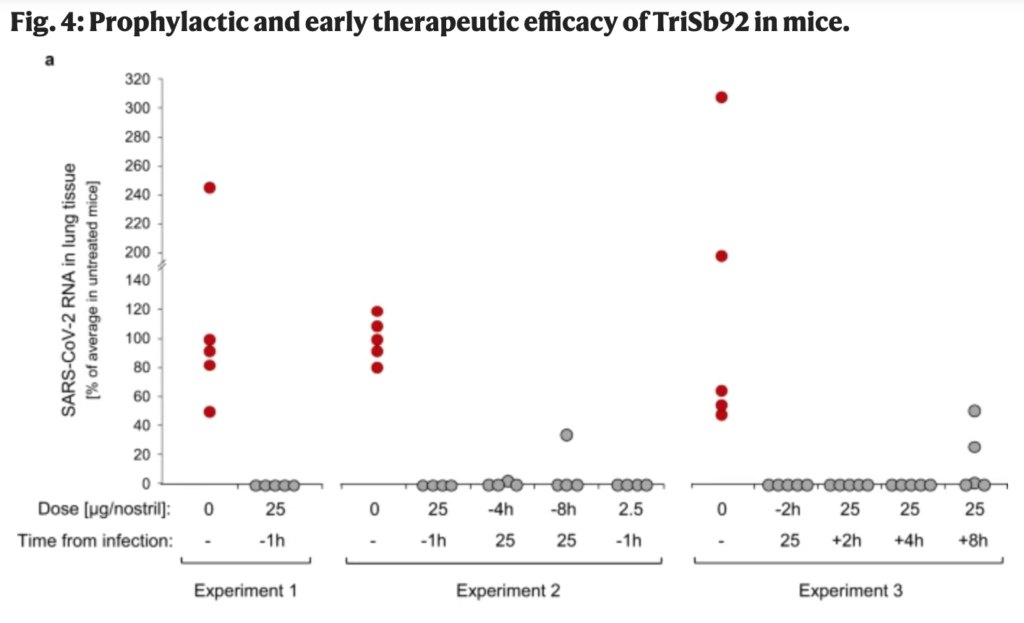
It seems strange to me that an airborne pathogen can be stopped at the nose — what about people who inhale it into the lungs? — but it sure seems like the nose is where the action is. As I mention on my Treatments page, there are bunch of nasal treatments which help prevent COVID-19 and/or shorten the recovery period: saline, nitric oxide, astodrimer sodium, a monoclonal antibody, and even blue dye+light.
This article from the UK says that 2.7% of the population had COVID-19 last week. They have a lower rate of people “fully vaccinated” (75% to 83%, with the difference being most pronounced in the younger age groups).
This Statistics Canada report says that in blood samples collected randomly from Canadian adults between April and August 2022, basically everybody (98.1%) had antibodies to spike (from infection or vaccination), while 53.9% had antibodies to the nucleocapsid (thus only from infection). This is in line with the 56.8% having nucleotide antibodies at the beginning of August 2022 in blood donors (as reported by a Canadian Blood Services report). While blood donors are not a perfect sample — they tend to be slightly healthier, more female, and I think whiter, and more affluent than the population as a whole — this makes me feel like using blood donor data will be at least close to the population as a whole.
Thus I tried to use blood donor data to estimate what the fraction of Canadians who are contagious with COVID-19 is. I failed, but I’m including my work below. You probably want to ignore it and skip down to Recommended Reading.
%Contagious Calculations
In the second week of January, this report said that 76.23% of Canadians had infection-acquired antibodies. This went up to 77.31% in the second week of February. This means that 1.08% of Canadians got their first COVID-19 infection in those four weeks, or about 4.5% of the people who had never been infected before.
That means that slightly more than 1% of those who had never been infected before got infected each week. Because people are infectious for about a week, that means that about 1% of previously-uninfected people are contagious at any given point.
Now, the people who had not been infected are probably more cautious and engage in more mitigation measures (like not eating in restaurants), and so those people are less likely to get exposed. How much less likely? (This is going to vary wildly from person to person, so you’d have to look at a population-level risk.) Let’s say that X is the exposure factor — how much more likely someone non-infected is to get exposed than the previously-infected.
People who had vaccinations and infections are less likely to get infected than people who were either vaccinated or infected then exposed, although both protections wane. According to this meta-analysis, the VE of hybrid immunity versus vaccination-only went from 69% at three months to 41% at twelve months. That means that the prercent of previously-infected people who have been re-infected and are now contagious is going to be between ~1%*X*31% and ~1%*X*59%, or between .3X% and .6X%. If X is 1, that means 0.3% to .6%; if X is 10, that means 3% to 6%.
Adding in the people getting infected for the first time, and if X is between 1 and 10, you have a total of (20%*1% + 80%*(.3% to 6%) = 0.2% + (.24% to 4.8%), or .44% to 5.0%. That range so big that it’s not really useful. 🙁
If you think have a good way to estimate X, let me know.
Recommended Reading
This article talks about vaccine hesitancy, and makes the point that adults were not in the habit of getting preventative vaccines, only reactive vaccines (like when stepping on a rusty nail). Preventative vaccines are for kids, right?
This blog post is kind of a review of what helps prevent Long COVID. tl;dr: don’t get COVID-19 (reduces Long COVID risk by 100%), take metformin (42% reduction), get vaccinated (43% reduction), take Paxlovid (26% reduction). Studies on treating with Paxlovid and with low-dose naltrexone are in process.
This opinion paper from the US talks about why TDF — a very cheap, very safe antiviral which had very promising effects against COVID-19 — did not get the trials it would have needed to get approved. tl;dr: It is a generic, so no company was going to fund the trial; the really good retrospective, observational data got ignored because of a bias towards random clinical trials.