
Long COVID
This preprint and this lay article report on a big US study of mental health effects after COVID-19 which found that people who had had COVID-19 had (compared to controls):
- 1.35x risk of anxiety disorders;
- 1.39x risk of depressive disorders;
- 1.38x risk of stress and adjustment disorders;
- 1.55x risk of antidepressant use;
- 1.65x risk of benzodiazepine use;
- 1.76x risk of opioid prescriptions;
- 1.34x risk of opioid use disorders;
- 1.20x risk of non-opioid substance use disorders;
- 1.80x risk of neurocognitive decline;
- 1.41x risk of sleep disorders.
Overall, people who had had COVID-19 had a 1.6x risk of having any mental health diagnosis.
The risks were higher for people who had been in hospital for COVID-19 vs controls, and they were also higher than vs. controls who had been in hospital for other causes.
Vaccines
This blog post (by a respected doctor) points to many studies which say that infection-acquired immunity is better than vaccine-acquired immunity, and argues forcefully that people who have been infected should get credit for it on vax cards and mandates. (My memory is that there have been a fair number of studies which show that vaccine-acquired immunity is better than infection-acquired immunity, but I don’t have time right now to chase down the references.) The blog author does acknowledge that the level of protection from infection-acquired immunity is much more variable than vaccine-acquired immunity, and that there is some selection bias: there was nobody in the study who had died of COVID-19.
The author also says that prior infection is not as effective against Omicron infection as two shots of vax, but he still thinks prior infection should count as 1 shot of vaccine.
He poo-poos people who say that giving people as much credit (for vax cards and mandates) is a bad idea. Me, I am leery of accepting prior infection on the vax card or mandate. How do you get it verified, especially if you had a private test? What about now in BC, when most people can’t get a PCR test? Are nucleotide antibodies enough? If they are, then I could game the system by getting a blood transfusion from my buddy who had COVID-19, which would make it look like I’d had prior infection. If a PCR test is enough, that means that there’s a possibility of fraud not just with the vax card but also with forging PCR tests. The vax card is a government document, so the penalties are probably higher for forging information there than on forging a PCR test. Etc.
Furthermore, with a bit of digging, I found that a serology test is $75. (And they probably aren’t 100% accurate.) The cost of a vaccine varies, but I believe that mRNA vaccines now cost about $15.
This paper looked at reinfections among people in Israel who had gotten COVID-19. They compared those who later (between March 1 and November 26, 2021) got a vaccine against those who did not. The vaccine effectiveness against infection was 60% for those over 65 compared to those who had prior infection and did not get vaccinated afterwards. Vaccination was 82% effective for those under 65. However, no significant difference in vaccine effectiveness was found for one dose as compared with two doses (which bolsters the argument of the prior blog post).

This paper from the UK reports that Pfizer with a long dose interval was 85% effective against infection 14-73 days after the second dose but fell to 51% effective at a median of 201 days. People who had infection-acquired immunity also had waning, but those who got vaccinated after their infection had effectiveness which was consistently higher than 90%, even 18 months after their infection.

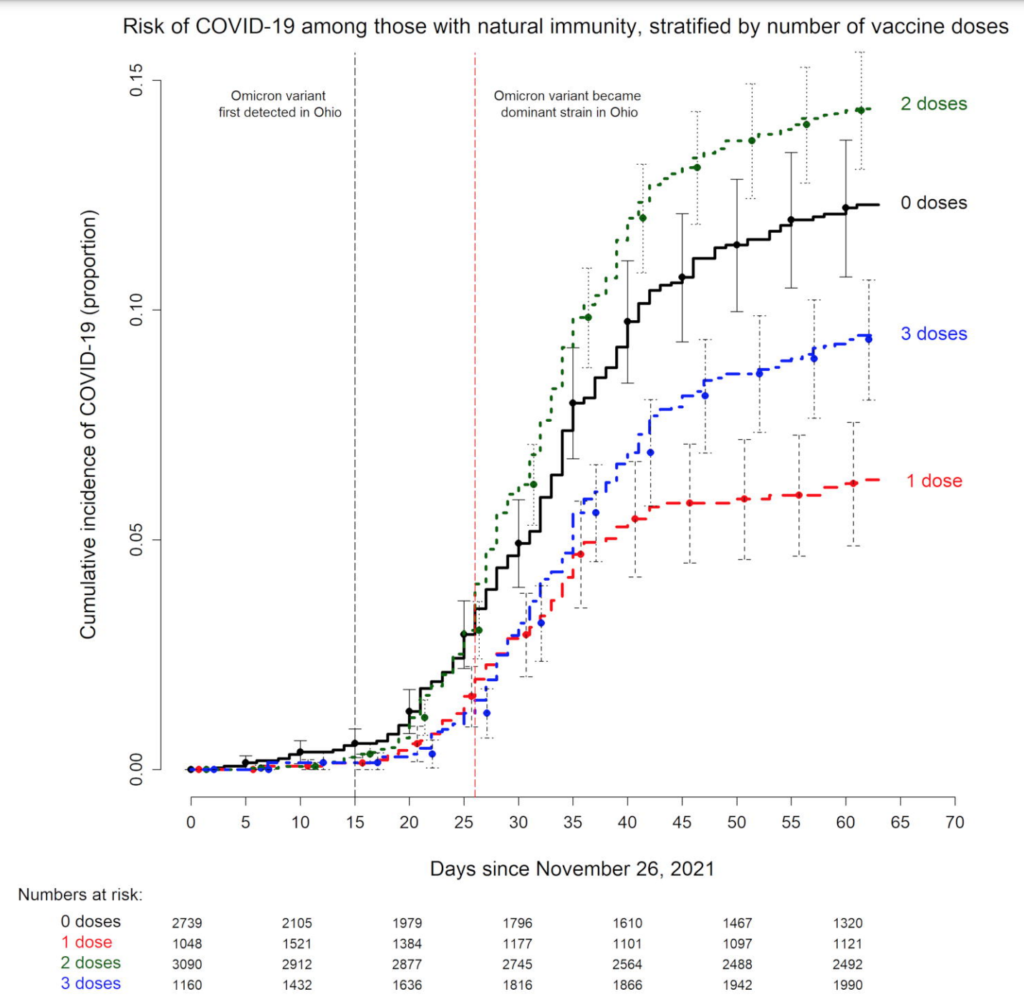
This preprint from Ohio found, among other things that I’m running out of time to tell about, that for people with prior infection, two or three subsequent doses was worse than one dose! Two doses was even worse than zero doses. This seems really really strange to me — part of me is yelling that I shouldn’t even post this because it’s so obviously a mistake — but Other Me says it might turn out to be real, so I should post it.
It might have something to do with which strain they got infected by. In order to have gotten three doses by the time the study was published, maybe that meant they needed to have gotten their booster early enough that their prior infection was Alpha and not Delta, and maybe Delta infections give better protection than Alpha infections.
Here’s another update from the UK on vax/booster effectiveness. Here’s the effectiveness against hospitalization:

Transmission/Pathology
This article investigates why Canada has fared so much better in the pandemic than the USA. From Our World In Data, the US has had ~78M cases (~240 cases per thousand), while Canada has had ~3.2M cases (~83 per thousand). BC has had ~340K (~68 per thousand).

Similarly, the peak ICU rate in the US was ~79/million, while it was ~32/million in Canada (and I think ~29/million in BC).

The death rate in the US has been ~279 per 100K, while the Canadian death rate has been ~94 per 100K (and ~55/100K in BC).
The article says it is because of:
- Better vaccination: 80% fully vaccinated/5% partially in Canada versus 64%/12% in the US (and 84.5%/5% in BC);
- Universal healthcare;
- Stricter mitigation measures for longer.
This has come at the expense of higher unemployment: 6.5% in Canada vs. 4% in the US (and 5.1% in BC).
Recommended Reading
This article is about pandemics and how they end.
This article talks about long-term medical consequences of previous epidemics (e.g. Long Polio, Long Epstein-Barr, etc.).
This article talks about what implications of the existence of both COVID-19 and immunocompromised people means.
This article describes different ways which the SARS-CoV-2 virus could evolve, and most of the ways are not pretty.