
I want to remind people again to get a flu shot this year. There’s a new substrain — H3N2 subclade K — which apparently is more contagious and nastier if you catch it. The flu shot isn’t hugely effective against infection but it has some effectiveness (especially for children!), and even if it doesn’t stop you from getting infected, it ought to make being sick suck a bit less.
General
Recommended Reading
This interview from Netherlands (2025-11-03) (which is in Dutch, you’ll need to run it through translation software) makes the argument that mental illnesses and the immune system are linked bidirectionally. For example:
- People with mental illnesses do not respond to vaccines as well as people without;
- About a third of people treated with interferon for Hepatitis C developed depression;
- people with several autoimmune diseases are at higher risk of depression and vice versa: if you treat the autoimmune disease, the depression gets better;
- people who in the hospital a lot with infections as a child have a higher risk of mental illness later in life;
- people with psoriasis, type 1 diabetes or rheumatism are at higher risk of psychiatric conditions, such as depression. And vice versa: when the autoimmune disease is treated, depression often decreases.
Vaccines
Before I started this blog, I knew that Guillain-Barré Syndrome (GBS) was a rare side effect of vaccination. Something that I had not realized was that GBS is also a rare side effect of infections. For example, this paper from USA (2025-11-14) reports that the risk of GBS doubles after someone catches RSV.
COVID-19
Long COVID
This paper from Canada (2025-09-29) reports that the vaccine effectiveness (VE) of a booster dose was 57% against Long COVID, though it waned after six months. They found that hybrid immunity’s (infection plus two to five vaccinations) effectiveness was 80% to 90% and did not vary by the number of doses or time since vaccination (up to 9 months).
If the hybrid effectiveness really is that good and doesn’t drop over time, then I would expect that the number of Long COVID cases would have dropped significantly over time. This, however, is contradicted by these papers:
- This article (2025-08-13) about this large, well-done paper from USA (2025-02-05) says that the number of Long COVID cases per COVID-19 case is actually rising.
- This paper (2025-05-08) from Australia found no significant difference in the likelihood of long Covid between the Omicron and pre-Omicron periods.
- This article (2025-08-25) about this paper (2025-02-05) from USA reports that the number of Long COVID cases per COVID-19 infection is going up.
This paper (2025-11-07) found that giving mice part of the COVID-19 spike protein (S1) intranasally quickly led to S1 in the brain, leading to cognitive dysfunction. Metformin made the cognition better.
The alert reader might note that all of the North American vaccines put spike proteins into the body. This is true but:
- Injections into the deltoid muscle are supposed to drain into the lymph system, not the circulatory system;
- you are going to get COVID-19 spike proteins into your body whether you like it or not. Either you can get it in a controlled fashion from vaccines, or in an uncontrolled fashion from a COVID-19 infection.
This paper from Ukraine (2025-09-21) reports that among children with Long COVID, symptoms dropped over time:
- 85.8% of patients at 3 months;
- 56.1% at 9 months;
- 32.5% at 12 months.
(I don’t understand how you could have only 85.8% at 3 months, because most definitions of Long COVID say that you have to have symptoms for three months!)
- The most common symptoms reported were fatigue, reduced physical activity, and headache.
- Older kids were more likely than younger kids to have decreased physical activity, lack of energy, neurological symptoms, headache, memory impairment, difficulty communicating, difficulty concentrating, cardiological symptoms, sensory symptoms, and dizziness.
- Younger children were more likely to have insomnia than older kids.
- Girls were more likely to have lack of energy than boys.
COVID-Related Excess Death and Sickness
This paper from Japan (2025-09-26) reports that people were five times more likely to get shingles in the week after a COVID-19 infection than in a period before infection. It dropped quickly after that first week, but there was still a 50% higher risk in weeks 5 and 6.
Treatments
This article (2025-11-14) discusses a new randomized clinical trial of a GLP-1 drug (tirzepatide, trade name Zepbound) against Long COVID. It explains that, yeah, GLP-1 drugs are mostly known for helping people lose weight, but that GLP-1 drugs also have generalized anti-inflammatory effects which might help Long COVID patients. The article calls out a paper from USA (2025-09-15) which found that 89% of people with Mast Cell Activation Syndrome — which shares some symptoms with Long COVID — found clinical benefit.
This paper from Scotland (2025-11-10) reports that among people who had been hospitalized with COVID-19, people who did resistance training five days per week had a higher quality of life than those who did not.
This seems like a bit of a “well, duh” study. I presume that resistance training improves EVERYBODY’S quality of life and the people who successfully kept up with the resistance training were the people who were healthier!
Addendum 2025-11-27: this blog post (2025-11-25) kind of eviscerates this paper.
This paper from USA (2025-11-10) reports that brain training software (BrainHQ) had no benefit vs. controls in improving cognitive function in people with Long COVID, including when coupled with direct current stimulation. This is in direct contradiction to a different study from Brazil (which I posted about in August 2025) which said that BrainHQ plus direct current stimulation did help quite a bit. Go figure. 🤷♀️
Pathology
This paper from Egypt (2025-11-12) reports that people with periodontitis were more likely to have had COVID-19 recently:
- People with higher clinical attachment loss (a measure of how far the gum has pulled away from the teeth) were 3.25 times more likely to have had COVID-19 recently than those with low values;
- people who had more bleeding-when-probed were 30% more likely to have had COVID-19 recently than those with less bleeding.
It was not clear to me which direction the causation was: did COVID-19 cause people’s gums to be less healthy, or did poor gum health make it more likely that people would catch COVID-19?
Testing
This paper from Germany (2025-10-12) says that “only 14% of those who tested PCR-positive actually became infected with SARS-CoV-2”. They acknowledge that PCR tests do recognize COVID-19 virus pieces that have gotten into the nose, but are suggesting that the virus frequently gets stopped in the nose, before it can actually infect the person.
However, they base that on measurements of IgG in the blood (AKA seropositivity), assuming “that the IgG-positive fraction is a practical proxy for prior infections” — but IgG measurements are also fallible!
I also suspect that there is also some form of sample bias: who was getting IgG tests (and why)? (There also were a lot more PCR tests than IgG tests — the most IgG tests per week was ~110,000 while the most PCR tests per week was ~3,000,000.)
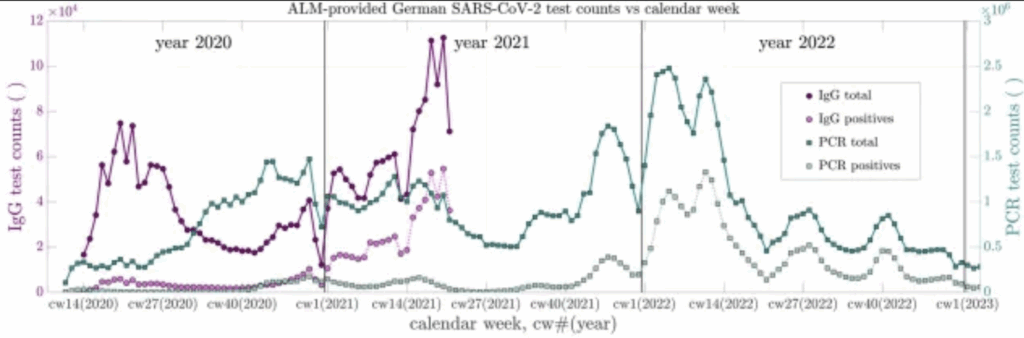
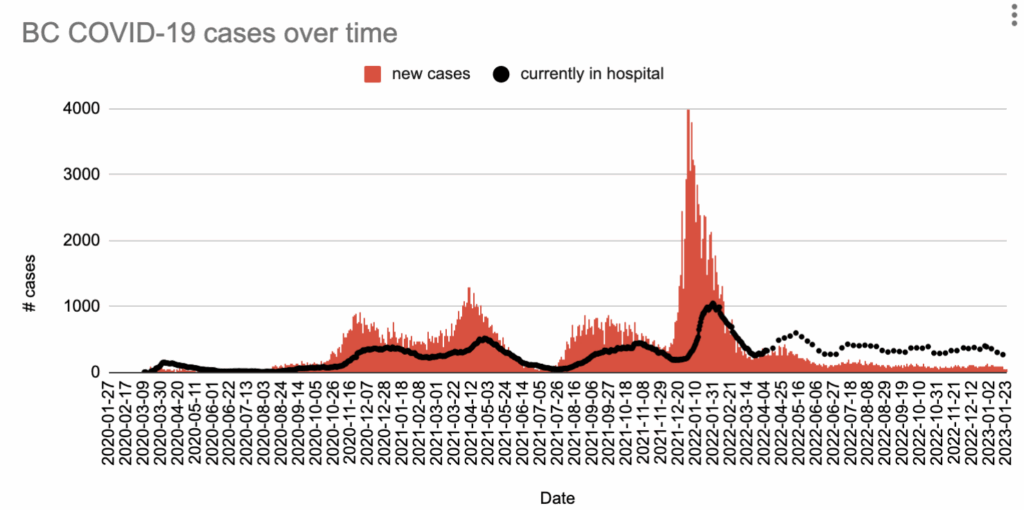
Their data also looks a little funny. Note that the count of IgG samples (purple) halts abruptly in late Spring 2021, and the spike of tests in the Omicron wave (early 2022) doesn’t reflect how large the Omicron spike really was, unless the Omicron spike in Germany was really really different from the Omicron spike in BC:
My spouse asked why I even print snippets about potentially flawed papers like this. It’s because you might see something about this paper, or have someone say, “oh, this paper says that people don’t actually get sick from COVID-19” and I want you to have tools to tell them why that’s bullshit have a more nuanced conversation with them.
One of the questions that this article brings up is “What does the word infection even mean?” If a virus gets into my body but does no damage and I can’t pass it on, am I “infected”? How far into my body does it need to get? Or is a provocation of my immune system enough to mean that I am “infected”? But how much of the immune system needs to react?
I have gotten four measles vaccinations in my life. Measles isn’t going to make me sick. But if I am exposed to measles, I believe that I won’t get sick because my immune system will rally and fight it off before I get symptoms. Now: would that count as a measles infection? Why or why not?
If you know somebody who actually knows what “infected” really means at a deep fundamental level, could you please have them contact me? I’m really curious.
Vaccination
Ed Yong once said that “immunology is where intuition goes to die”. I thought of that when I read this press release about research presented at a conference (2025-11-06): it reported that among children with eczema, those who got a COVID-19 vaccination had lower risks of many many illnesses:
- ear inflammation (otitis media) – 38% lower risk;
- pneumonia – 40% lower risk;
- bronchitis – 52% lower risk;
- non-COVID viral infections – 45% lower risk;
- sinusitis – 45% lower risk;
- upper respiratory infections – 35% lower risk;
- impetigo – 51% lower risk;
- molluscum contagiosum – 40% lower risk;
- skin infections – 44% lower risk;
- asthma – 30% lower risk;
- allergic rhinitis – 44% lower risk;
- contact dermatitis – 46% lower risk;
- other allergy-related risks – 30% lower risk.
Why on earth would a COVID-19 vaccination reduce the risk of a skin infection??? WTF?
This article (2025-11-10) about this (paywalled) paper (2025-09-29) using data from Nebraska in late 2024 and early 2025 found that the vaccines in use then were effective against COVID-19. Vaccine effectiveness at four weeks was:
- 44.7% against infection
- 45.1% against Emergency Department visits;
- 57.5% effective against hospitalization or death.
Effectiveness against infection waned down to 35.0% at 10 weeks and 16.7% at 20 weeks.
Influenza
Testing
This article from USA (2025-11-12) makes a passing mention of the fact that the US CDC hasn’t published respiratory surveillance data about the flu since September 26 due to the massive clusterfuck challenging times in the USA federal health agencies. This affects us in Canada because it means we have less information about and a lot less analysis of what is circulating in our nearest neighbour. Yes, the US federal shutdown is over, but I don’t know how long it will take for the data to flow again.
Caitlin Rivers and her team at Force of Infection have been collecting influenza data from every US State health website and interprets the data holistically. Her most recent report says that in most places in the US, influenza levels are still low but starting to move up.
Vaccines
This preprint of a report from UK (2025-11-12) says that H3N2 subclade K is dominant in early flu cases there, but despite K being a poor match for the H3N2 subclade J.2 in this year’s flu vaccine, the vaccine is still managing to give the typical range of 70 to 75% in children and 30 to 40% in adults.
RSV
Vaccines
This paper from England (2025-10-27) reports that in people ages 75-79, the RSV vaccine was 82.3% effective against hospitalization for RSV.
Epstein-Barr Virus
Pathology
There was a paper from USA (2022-01-24) which pretty conclusively linked Multiple Sclerosis to the Epstein-Barr Virus (EBV), and now this paper from USA (2022-11-12) has linked EBV to lupus! I hope/expect that this paper will add additional motivation to come up with an EBV vaccine!
There was also a recent paper (2025-10-14) which found that rates of Multiple Sclerosis and ALS are correlated. (Addendum: this paper from Sweden (2026-01-20) reports that air pollution also raises the risk of ALS.)
Meanwhile, there are hints that Long COVID and ME/CFS might be related to EBV.
And of course, EBV causes mononucleosis.
Wouldn’t it be nice if we could get rid of MS and Long COVID and ME/CFS and lupus and ALS and mononucleosis by vaccinating against one virus??
Addendum 2025-11-20: This article (2025-07-10) reports that scientists have found links between EBV exposure and a number of different cancers.
Addendum 2025-11-25: This paper (2021-10-27) lists the following cancers as being associated with EBV: nasopharyngeal carcinoma, gastric carcinoma, Hodgkin lymphoma, Burkitt lymphoma, diffuse large B-cell lymphoma and xxtranodal NK/T-cell lymphoma/nasal type.
H5N1
Transmission
This review paper (2025-10-29) reports that there have been sixteen identified cases of asymptomatic H5N1 cases in humans globally: 8 in Bangladesh, 3 in Vietnam, 2 in Cambodia, 2 in Spain, and 1 in the UK. These cases were found by testing people who had been exposed to H5N1-infected people. (Yay, contact tracing!)
Measles
Transmission
According to the Government of Canada Measles and Rubella Monitoring Report (updated 2025-11-10), in the week ending 1 November, the following jurisdictions had the following number of cases:
- Canada: 23;
- BC: 12;
- Manitoba: 9;
- Alberta: 2.
1 comment
Comments are closed.