
Long COVID
This preprint from USA says they used PET scans to look at inflammation in the brains of long haulers, and found more inflammation in long haulers than in controls.
This preprint from many places says that they found evidence of reactivation of herpesvirus type 6 in long haulers (mostly a childhood disease, where it causes a rash).
Wow! This paper from UK says that Long COVID rates have dropped dramatically since COVID Classic. I believe the y-axis is the percentage of people who recovered in the (x-axis) number of weeks.
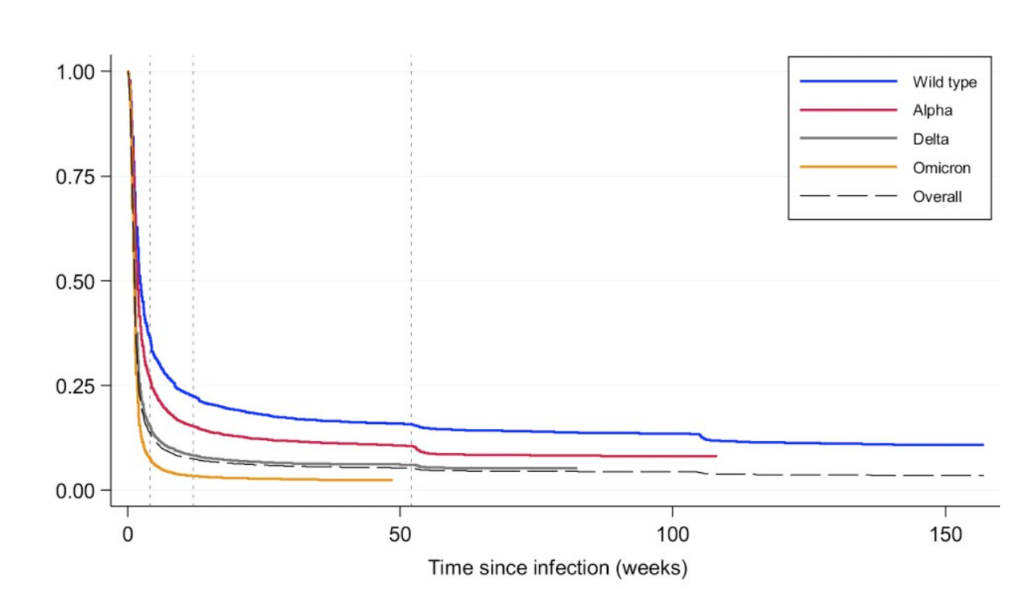
Some of this might be that the most susceptible to Long COVID were also most susceptible to COVID, so they got COVID and Long COVID right away, so the proportion of people who got the infection for the first time is going to keep falling over time.
This paper from Sweden looked at cerebrospinal fluid for SARS-CoV-2 and a ton of other markers (especially ones associated with inflammation and/or damage) for people who had had COVID-19 infections and controls who had not. They found no SARS-CoV-2 in the brain and no differences in the other markers. This is good news! If this holds up (which it might not — brain autopsies have found SARS-CoV-2 in the brain), that might mean that Long COVID is reversible!
This paper from USA says that Paxlovid decreases the risk of Long COVID by 13% and molnupiravir by 8% compared to no treatment. There was a significant gender difference, with men getting the better deal: with Paxlovid, men decreased their risk by 16% and women by 11%. With molnupiravir, men decreased their risk by 12% vs. 5% for women.
COVID-Related Excess Deaths and Sickness
This spreadsheet lists papers which have found long-term negative health effects of COVID-19 infections. There are currently 312 studies on the list.
Transmission
This paper from USA found that kids were infectious for about three days, and it didn’t matter how many vaccination shots they’d had.

Vaccines
This paper from USA found that the COVID Classic vax waned so much that after ~7 months, it had practically zero effectiveness (red points) against infection, and only 28% effectiveness against hospitalization. Getting a bivalent BA.5 booster also didn’t give fantastic protection, but it was a lot better — 59% vaccine effectiveness (blue dots, lower graph) against hospitalization.

The paper also found that the bivalent BA.5 booster was better than a BA.5 infection when it came to hospitalization. Infection was about the same as the bivalent BA.5 booster when it came to emergency/urgent care visits or infection.
| Effectiveness against | BA.5 booster | infection |
| hospital admission | 56% | 40% |
| ED/UC visit | 34% | 36% |
| outpatient encounter | 29% | 27% |
This paper — and especially how it has been interpreted in e.g. this article — implies that vaccine passports were not much good because they didn’t lead to much more vaccination, as if vaccination in and of itself was the goal. I supported vaccine passports because I wanted to be safer in places like restaurants! (This was back when we thought vaccines would keep you from getting sick, sigh. Those were the days.)
Babies whose mothers were vaccinated against COVID-19 fared better than those whose mothers were unvaccinated:
| risk | vaxed mom | unvaxed mom |
| Severe Neonatal Morbidity | 7.3% | 8.3% |
| neonatal death | 0.09% | 0.16% |
| NICU admission | 11.4% | 13.1% |
This preprint from USA looked at stroke risk after getting a bivalent vaccination. They found that there was only a risk for people over 85. In the three subsequent weeks after getting a Pfizer bivalent vax, people over 85 had a 36% higher risk of a non-hemorrhagic stroke (NHS) and a 28% higher risk of a transient ischemic attack (TIA).
Among those who got a high-dose flu shot and a COVID-19 bivalent shot at the same time, people who got Pfizer+flu hd a 20% higher risk of an NHS. People who got Moderna+flu had a 36% higher chance of getting a TIA.
I have no idea why your risk would be lower if you got the Pfizer+flu than if you got the Pfizer only.
People who only got a high-dose flu shot had a 9% higher chance of getting an NHS.
(NB: Getting a flu shot cuts your risk of heart attack in half for the next year. Getting COVID-19 increases your risk of all kinds of things, including cardiovascular and autoimmune diseases. Don’t skip your boosters!)
I thought this graph of deaths over time in the USA from this article was interesting. There were WAY more Omicron cases than Delta cases, but the deaths weren’t THAT much higher. (And for Pacific Islanders, deaths were lower for Omicron.)

Variants
This paper from USA says that SARS-CoV-2 has been mutating at a rate 2 to 2.5 times faster than influenza (which previously was by far the fastest-mutating disease). Note that they talk about the mutation rate “per year” as opposed to “per case”, so if I understand correctly, the mutation rate is going to be influenced by how many people catch it per year. If 2.5x as many people catch COVID-19 as catch influenza, then if they have the same mutation rate per case, then you’d expect the mutation rate per year to be 2.5 times as high for COVID-19 as for influenza. So how many people catch each in a year?
Well, that’s really difficult to say because testing for both is pretty lame. But from this BC CDC graph of samples from doctor visits for upper respiratory infections, it looks like flu peaked 2x higher last year, but COVID-19 is much more common throughout the year:
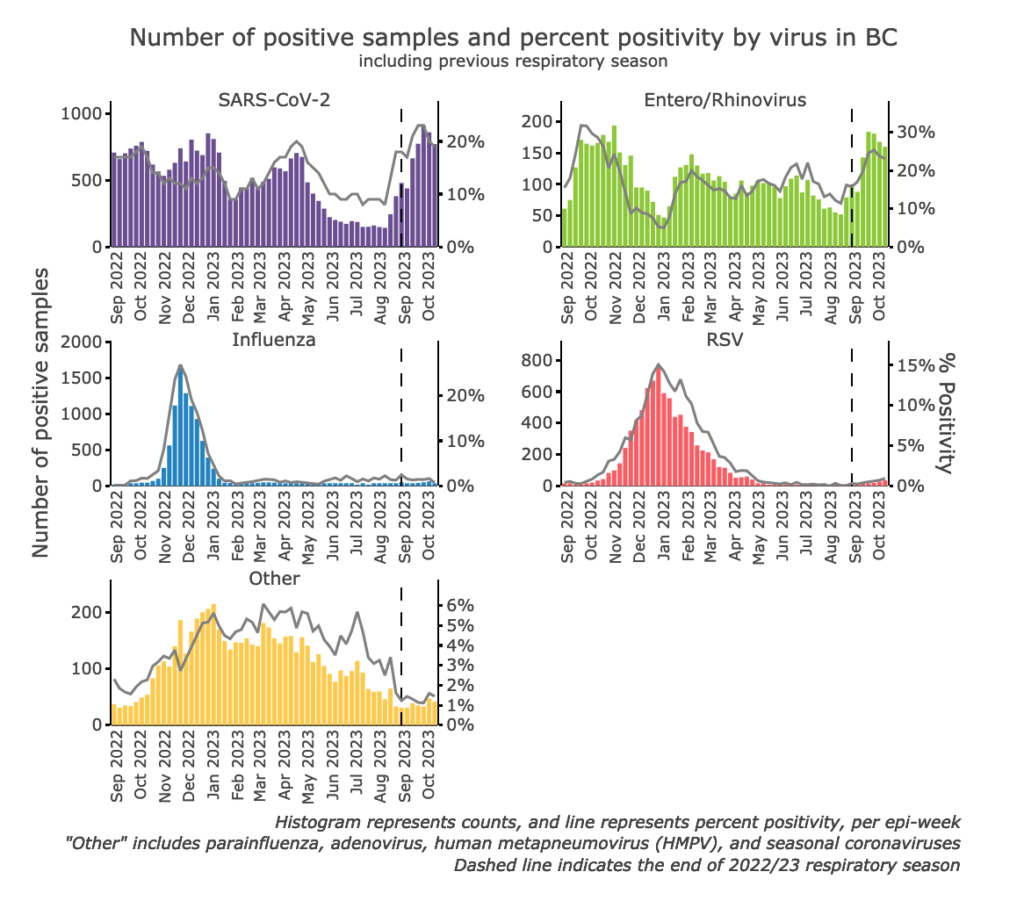
My eyeball guesstimate integration under the curve says that there were about 7100 COVID-19 cases in the 13 months covered by the above graph, while I estimate about 2550 influenza cases — or 2.8 times as many COVID-19 cases as influenza cases. That implies that the mutation rate of COVID-19 per case is slightly less than the influenza mutation rate per case.
Treatments
This paper from Belgium says that people who were on ventilators from COVID-19 ARDS died less if they got an infusion of convalescent plasma (35.4% mortality, 32.7% if they got the infusion before 48 hours after going on the ventilator) than people who got standard care (45% mortality).
This paper from Canada found that 70% of patients (with a median age of 70) getting Paxlovid were taking a drug with a known drug-drug interaction. They kept the other medication in 56% of the cases (with the majority of those being statins), adjusted the dose in 22% of the cases, and switched to a different drug in 8% of the cases.
The good news is that only 1.2% of the patients were hospitalized with COVID-19, and there were zero deaths. 😀
Pathology
This paper from UK found that people with severe mental illness were 53% more likely to die from a COVID-19 infection than controls were.
This paper from USA found that people with HIV were 46% more likely to get a COVID-19 reinfection than controls were.
Recommended Reading
This article from USA asserts that teaching has changed because the kids are changed, traumatized by the moral responsibility of wearing masks, of loved ones dying, of their parents losing their jobs, of them and/or their parents having long-term consequences of COVID infections.