
I want to talk for a moment about human metapneumonia virus (HMPV). It is NOT some strange new virus which is killing people in China — again. HMPV has been circulating for at least sixty years, I have almost certainly had it, you have probably had it. BC has been tracking it for years: I have always seen it when I looked at the Pathogen Characterization page. (Three percent of the influenza-like illnesses which BC found in the week of 28 Dec 2024 were HMPV.)
HPMV is not new, it’s not scary. It’s a cold. Yes, you can have severe cases, but that’s unusual — just like severe cases from rhinoviruses are rare.
Why is China having so many cases right now? Possibly because COVID-19 messes up your immune system. It’s more likely because nobody caught it for a few years while China was under lockdown, so nobody had recent immune memory. That means everybody is getting it at the same time now. (We had the same thing happen on this side of the pond with RSV.)
This isn’t pandemic news, but it’s important to understand in the context of pandemics. There are a lot of people who think of the immune system like a muscle, that you have to exercise it regularly or it gets weak. A better way to think of it is as a reservoir that gets depleted more and more as it gets used.
This article (2025-01-06) on a study in Denmark reports that kids who get a lot of infections early in life have more trouble later in life: more moderate-to-severe infections later.
COVID-19
Long COVID
⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐
O. M. F. G.❗❗❗❗❗❗❗❗❗❗❗❗❗❗❗❗❗❗❗❗❗❗❗
LOOK AT THIS GRAPH! LOOK AT THIS GRAPH! LOOK AT THIS GRAPH OF PLACEBO VS. TREATMENT FOR DEVELOPING LONG COVID!
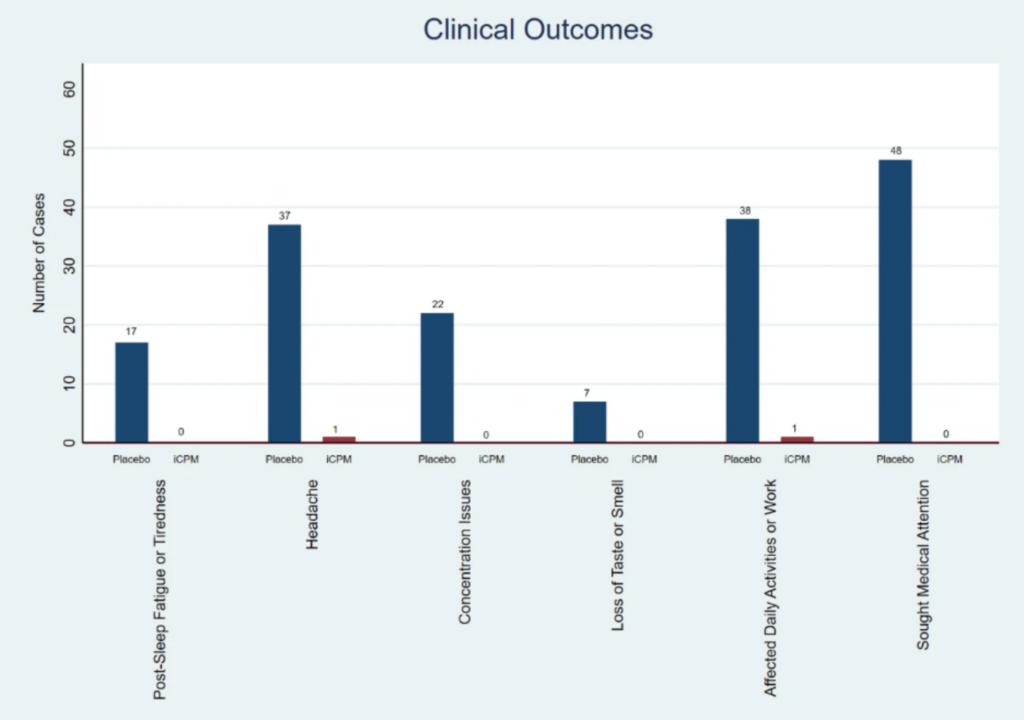
The bars are the number of people who developed Long COVID symptoms. The blue bars are people who got a placebo. The red bars (that you can hardly see) are people who got intranasal chlorpheniramine — an H1 antagonist antihistamine — right away after they tested positive for COVID-19.
(If you can’t read the labels (I know, the text is small!), they read Post-Sleep Fatigue or Tiredness, then Headache, Concentration Issues, Loss of Taste or Smell, Affected Daily Activities or Work, and Sought Medical Attention.)
This graph is from this paper using data from Honduras (2024-11-26).
What’s the catch? I don’t know. I do think it’s odd that I didn’t hear about a paper with results this astonishing for more than two months. I thought maybe it was because it was from Honduras, maybe people didn’t trust Honduran doctors? Except that ten of the co-authors are from the US and one is from Spain. The journal that it is published in is BMC Infectious Diseases, which is a reasonably well-respected journal, with an impact factor of 3.4 (second quartile). Maybe because one of the paper authors works for a company that distributes a chlorpheniramine nasal spray in Panama and Dominican Republic?
Do I believe this data? Yes, actually. There’s a lot of solid research for “stuff in the nose does good things”, there’s some good research for “H1 antagonist antihistamines do good things”, so it’s easy for me to believe that the combo is doubleplusgood.
So how can we get the benefit of this research? Errr… I’m not sure. There are oral versions of chlorpheniramine over the counter in Canada, but not intranasal versions. (Same in the USA, sorry, you can’t just sneak over the border to get some.)
I don’t know if a compounding pharmacy could put it in a bottle for you. I suspect they need a prescription, and I don’t know how to get a prescription for an over-the-counter drug.
If you can find a source, the dosage used in the paper was 100 µL of a 1.0% chlorpheniramine solution per nostril three times per day for ten days. (FYI, the study’s daily dose works out to approximately half of the daily maximum recommended oral dose.)
Practically every study on Long COVID remarks that women are more likely to get Long COVID than men are. Is this due to hormone levels? Having two XX chromosomes? Misogyny? This paper from USA (2025-01-02) reports that it’s not the hormones. They looked at transgender and non-binary people who had had COVID-19 infections, and found that Long COVID was most likely in people assigned female at birth, and that hormones didn’t affect Long COVID risk.
This article from USA (2024-01-02) reports on how the number of Americans with disabilities has “skyrocketed” since 2020:
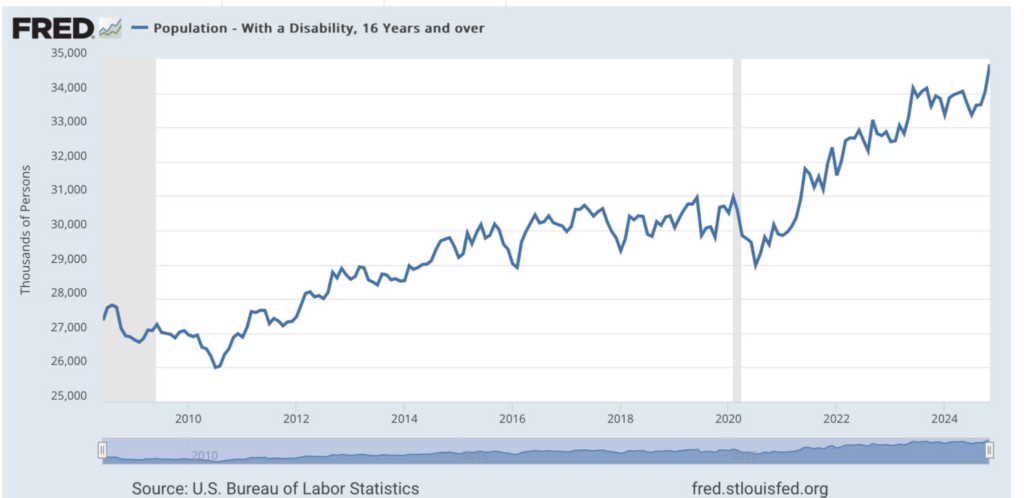
They attribute the jump to Long COVID, COVID-related excess sickness (e.g. more heart problems), lockdown-related isolation stress, loss of loved ones, poor ergonomics in work-from-home setups, and Boomers getting old.
This set of case studies from USA (2025-01-06) found that Long Covid patients who took a fifteen-day (or longer) course of Paxlovid did… well, variably. About 70% saw some improvement, but it only lasted for 38% of the patients. About 30% saw no improvement. Fortunately, nobody got worse. NB: this was a very small study — just 13 participants.
This paper from Spain (2024-10-01) reports that people with Long COVID had significantly lower verbal fluency than controls.
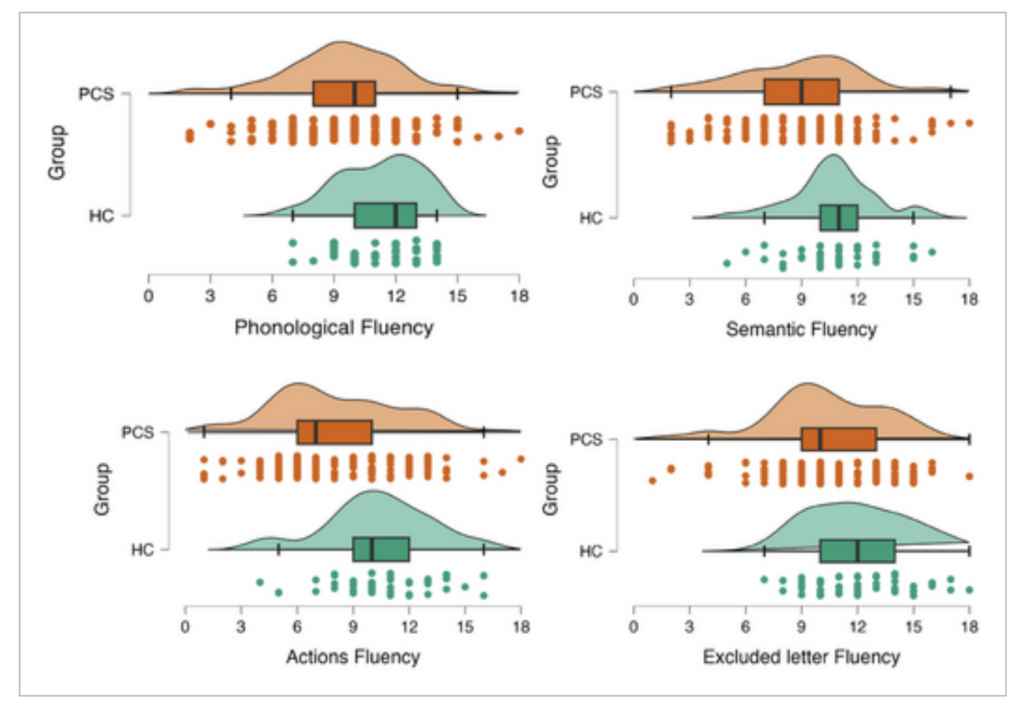
One wild thing: younger people with Long COVID did worse than older people with Long COVID. This was opposite from the healthy control cohort: older controls did worse than younger controls.
This paper from UK (2025-01-09) reports that vaccination helped some people with persistent symptoms. They looked at people who had Long COVID symptoms at 12 weeks from the onset of COVID-19 (which was presumed to be the Alpha variant because of the timing). Some of those people got better and then worse, and some just never got all the way better.
They found that some people who got vaccinated at least 28 days before symptoms started had a bit more improvement in their symptoms than people who did not, especially for cough, fatigue, and loss of smell:
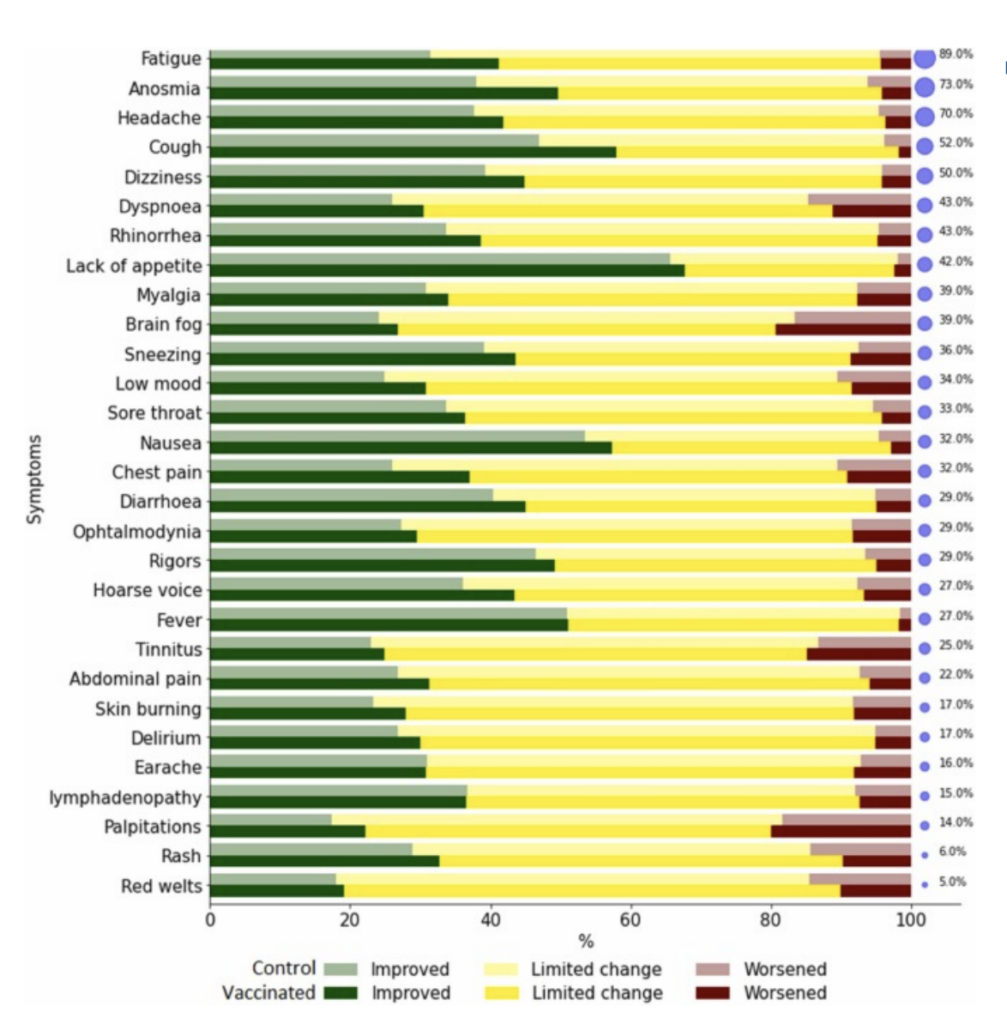
There were a few symptoms which were slightly worse in vaccinated people than unvaccinated.
They also looked at people who got a flu vax, and the flu vax did not have any effect on the Long COVID symptoms.
This paper from USA (2025-01-07) reports on risk factors for Long COVID found in a cohort of essential workers (mostly first responders). They quantified elevated risks for Long COVID:
- 41% higher risk for those who had multiple infections;
- 3.17 times higher risk for those who had severe COVID-19;
- 3.29 times higher risk for those who were unvaccinated at the time of their first infection.
Treatments
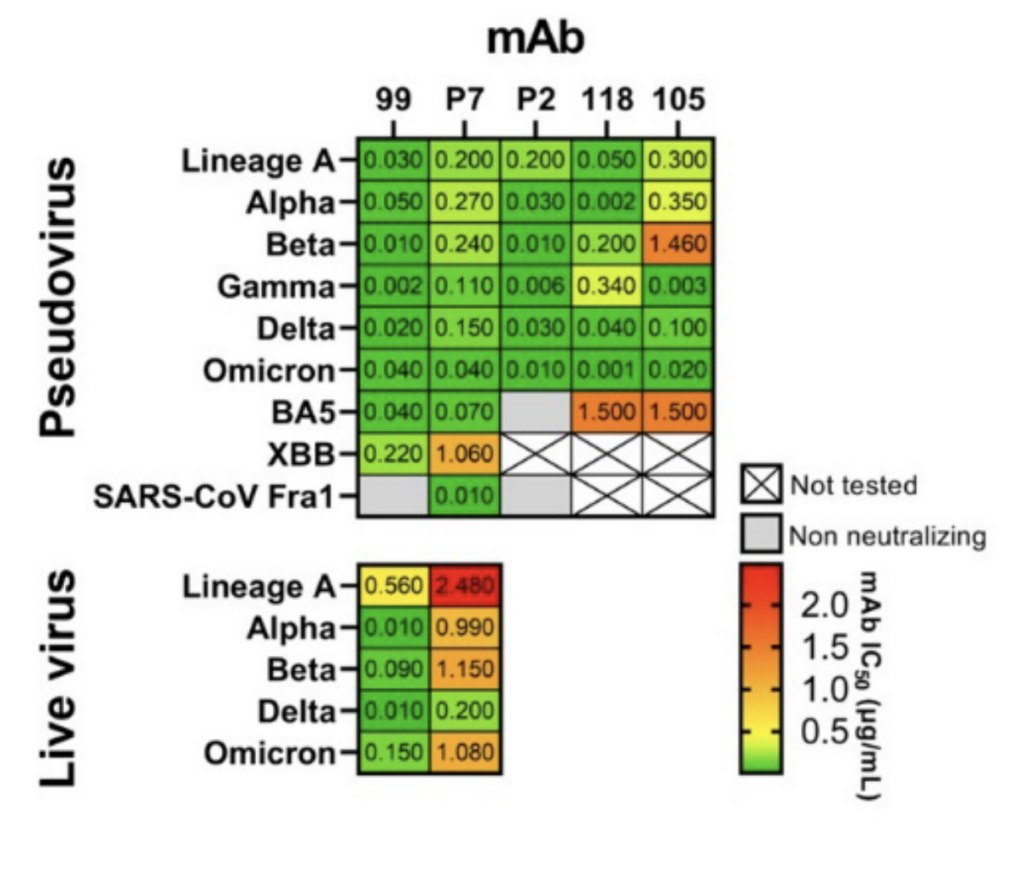
This preprint (2025-01-03) reports on monoclonal antibodies derived from cow antibodies.
The alert reader might remember that camels have really small antibodies (“nanobodies”); it turns out that bovines have really big antibodies. The authors vaccinated cows five times with various forms of the COVID Classic spike, and then examined their blood for good antibodies. They found a bunch of good antibodies and two freakin’ phenomenal antibodies, mAb99 and mAbP7. The mAbP7 antibody wasn’t quite as strong against the COVID-19 variants (especially XBB and live COVID Classic), but it neutralized SARS, which mAb99 didn’t.
I have no idea how easy it is to manufacture cow antibodies.
Older and/or poor Americans! The US Government will pay for all or most of your Paxlovid, but you have to know how to ask for it! See this website.
Vaccines
This preprint (2024-12-29) reports that the effectiveness of Pfizer’s KP.2 vaccine was:
- 68% against hospitalization;
- 57% against emergency room / urgent care visits;
- 56% against outpatient visits.
Remember that looks at the number of people who got sick during the study period compared to the number of people who got sick who did not get a KP.2 booster: that includes people who got other vaccinations and people who have gotten COVID-19 infections. If you instead compared vaccinated people to people who had never gotten a vaccination and had never gotten a COVID-19 infection, the VE would be much, much higher.
Mitigation Measures
While I believe that hospital-acquired infection rates rose during the first few years of the pandemic (sorry, I have no citation handy), mostly from COVID-19 infections, this paper from China (2025-01-03) reports that hospital-acquired infections went down by 20% in some cardiac care units! Maybe that’s because they were being really careful about COVID-19 and they did zero-COVID for a long time (which would have also cut down on transmission of every other infectious disease).
Pathology
This review paper (2024-09-24) reports that myopia went up a lot after the pandemic hit. That didn’t surprise me at all, because scientists have found (over and over!) that lack of adequate sunlight in one’s youth correlates with myopia. See this review paper (2021-03-18), for example.
H5N1
Pathology
This article (2025-01-06) reports that the Loiusiana case — who caught it from their backyard flock and who had underlying health issues — died. That’s the first death from H5N1 in North America (that we know of).
This Letter (2024-12-31) describes what the 46 US cases (through October) have looked like.
- 20 were exposed to infected poultry, 25 were exposed to infected cattle. The other person went into the hospital for something unrelated, and they only found the bird flu from normal surveillance. (I believe that was the first of the two Missouri patients.)
- All cases were mild, nobody died (remember, this is from October), and 87% received TamiFlu. (I don’t know if that’s the number who were offered TamiFlu, or the number who took TamiFlu.) The median time after start of symptoms that they were given TamiFlu was two days.
- 93% have had conjunctivitis, with 33% having only conjunctivitis;
- 49% had fever;
- 36% had respiratory symptoms.
- The illness lasted between 1 and 8 days, with a median of four days.
- The most common PPE used was:
- gloves (71%);
- eye protection (60%);
- face masks (47%)
Mitigation Measures
This press release (2025-01-08) reports that the US federal government has expanded its bulk milk testing program to 15 more states, for a total of 30 states. It also mentions that the bulk milk testing program has found zero cases of bird flu. If the bulk milk testing is done properly, that’s a really good sign. If the farmers are subverting the testing program or the USDA is messing up the testing, that’s a bad sign.
Vaccines
This press release (2025-01-08) from the US Department of Agriculture discusses vaccination of poultry and cattle. They say that vaccinating poultry would be “difficult in practice and may have trade implications”. Unpacking that, I suspect that vaccinating birds might be “difficult in practice” because there are a lot of birds.
It is possible to do large-scale vaccination; other countries have done it. Thus article (2023-11-06) mentions that Mexico has been vaccinating against H5N2 since 1995. This article (2005-11-16) reports in detail that China vaccinated 5.2 billion-with-a-B birds against H5N1 in 2005, and the the 2023-11-06 article says they are still doing vaccinations (and moved to a H5/H7 bivalent vax when H7N9 showed up). The 2005-11-16 article says that the vaccine costs ten cents per dose and “it is nearly 100 percent effective”.
As for “trade implications”, this article from USA (2023-04-06) says that some countries will not import eggs from vaccinated chickens.
Transmission
This article (2025-01-06) reports that there are now 917 dairy herds in the US which have ever been infected with H5N1, with 701 of the herds in California. This article (2025-01-09) mentions that 100 of the California dairy herds have come out of quarantine by now.