
Long COVID
This paper from UK (2024-03-01) found that the blood of people who just had a COVID-19 infection was measurably different between those that developed/did not develop Long COVID later. Specifically, the ones who later developed Long COVID showed lower levels of blood iron and more inflammation. It’s not that they weren’t eating enough iron — the body was actively sweeping iron out of the blood. (This is apparently normal when fighting off an infection to starve bacteria of iron; it’s just not supposed to persist.)
Please be clear that the anemia isn’t why Long COVID gives people fatigue: it’s a marker of problem. People who were anemic shortly after they recovered from COVID-19 were more likely to get Long COVID later. Yeah, it’s kind of a wtf.
Looking into iron some more, this paper in UK (2022-11-05) says they were doing study where they were giving ferric derisomaltose (basically an intravenous iron boost) to heart patients, and then the pandemic hit. They found that patients who had been given IV ferric derisomaltose had a 24% lower risk of being hospitalized or dying when they got COVID, compared to heart patients who got COVID who did not get the IV iron boost.
Meanwhile, this paper from Europe (2022-03-30) found that patients with thalassaemia (a genetic disorder which usually leads to anemia, and which is treated by boosting iron levels by infusion or iron chelation) had a lower risk of dying from COVID-19. Patients who had thalassaemia and COVID did better if they got blood transfusions. Maybe because their iron levels were watched so closely, their iron levels were higher than the average person?
It is also interesting that the demographic that has been hit the hardest by Long COVID — pre-menopausal women — is also the demographic which loses a lot of blood/iron for about a quarter of their weeks.
I will be keeping my eye on research about COVID-19 and iron from here on.
This (long! and very detailed!) paper from USA (2024-03-04) looked at sex differences in Long COVID. Men and women have different symptom profiles, and in general, women have it worse (see below image for comparative M/F histograms on symptom frequency, note that women are blue). The most common thing that women got that men didn’t was hair loss; the most common thing that men got that women didn’t was sexual dysfunction.

They also found that lower levels of non-dominant sex hormones correlated with Long COVID risk. Women with lower testosterone were more likely to get Long COVID.

In men, low levels of estradiol increased the risk of Long COVID:
They also used machine learning to find a cocktail of markers (excluding the sex hormones) that predicted Long COVID with ~86% accuracy:

They also found that having antibodies to HSV-2 (genital herpes) was a strong risk factor for Long COVID in women, and HSV-1 antibodies were a factor (though weaker) in men.
Testosterone seemed to be a little bit of a magic hormone: in general, the lower your testosterone levels, the worse your Long COVID symptoms were.
They found that lower testosterone levels correlated with higher levels of various herpesviruses antibodies (which presumably came from re-activation of the viruses), and which viruses had higher antibody levels differed between men and women.
(Interestingly, this study came about because a woman contacted one of the principal investigators to tell her about how much better her child’s Long COVID symptoms were after receiving testosterone for transitioning from female to male! Gender diversity for the win! Listening to patients for the win!
And before you ask, this article from USA reports that transgender people get Long COVID more than cisgender people.)
I wonder: I have seen a fair number of studies that have found clusters of symptoms. I now wonder how many of those clusters were “what-men-have” and “what-women-have”, and the researchers just didn’t ever think to pull men and women into two different subgroups. Maybe there aren’t Long COVID symptom clusters per se, just men and women reacting differently.
This paper from USA (2023-12-29) reports on four case studies. These patients at a Long COVID clinic reported that they had much worse reactions to alcohol than pre-COVID: worse hangovers, bad flushing, worsening Long COVID symptoms, etc.
This paper from USA (2024-03-08) found that vaccination provided some protection to kids from Long COVID.
- Vaccine effectiveness against probable Long COVID within 12 months was 35.4%; against diagnosed Long COVID, it was 41.7%.
- VE was 50.3% for adolescents but only 23.8% for 5 to 11 year olds.
- VE waned: 61.4% at six months but only 10.6% at 18 months.
Pathology
On the theme of gender differences, this paper from Liechtenstein (wow, go Liechtenstein!) (2024-03-06) used a smart bracelet to measure various physiological metrics. They found that men had significantly larger increases in skin temperature, breathing rate, heart rate, and larger decreases in heart rate variability than women when symptomatic with COVID-19. (They didn’t really know what it meant, though.)
This preprint from Qatar (2024-02-23) found that the protection given by previous infections against JN.1 virus (which is the dominant strain these days) is lower and lower as the previous infection gets farther and farther away. This is probably both due to waning immunity and to the virus mutating away from the previous infection.
The effectiveness of a prior infection against a JN.1 reinfection was:
| Months post-infection | Effectiveness |
| 3 to 6 | 82.4% |
| 6 to 9 | 50.9% |
| 9 to 12 | 18.3% |
| > 12 | 1.8% |
This paper from USA (2024-02-27) finds that vaccination during the follicular phase (i.e. not during the period) causes a temporary lengthening of the period for about a day. They did not find any effect when the vaccination was in the luteal phase. Women, you might want to get vaccinated when you are having your period.
COVID-Related Excess Sickness and Death
This paper from China using UK Biobank data (2024-02-17) found that risks for a variety of lung diseases goes up significantly after a COVID-19 infection:

Note: they looked at the risk over the time period of the study (between January 30th, 2020 and October 30th, 2022), so if someone caught COVID on Oct 29th, 2021, that person wouldn’t have time to get e.g. lung cancer. I’m not sure how that affects the numbers.
The risk was higher if the patients were hospitalized. The increased risk (versus contemporaries who didn’t have COVID) for various lung diseases over the course of the study was:
| Disease | Unhospitalized | Hospitalized |
| Asthma | 1.45x | 1.84x |
| Bronchiectasis | 1.10x | 3.13x |
| COPD | 1.48x | 2.00x |
| Pulmonary eosinophilia | 1.08x | 2.64x |
| Sarcoidosis | 1.71x | 5.97x |
| Pulmonary embolism | 1.16x | 3.82x |
| Pulmonary heart diseases | 1.08x | 4.31x |
| Pulmonary edema | 0.86x | 7.48x |
| Lung cancer | 1.18x | 2.18x |
But wait, it gets worse! They actually had two different control groups; the one above was contemporary controls. If they used pre-pandemic data for their controls, the numbers frequently got significantly worse:
| Disease | Unhospitalized | Hospitalized |
| Asthma | 1.31x | 1.65x |
| Bronchiectasis | 1.35x | 4.02x |
| COPD | 1.35x | 1.97x |
| Pulmonary eosinophilia | 1.26x | 3.23x |
| Sarcoidosis | 1.90x | 5.74x |
| Pulmonary embolism | 1.83x | 6.17x |
| Pulmonary heart diseases | 1.76x | 4.31x |
| Pulmonary edema | 0.95x | 11.58x |
| Lung cancer | 2.01x | 3.94x |
Yes, you read that right: if you are hospitalized with COVID-19, your risk of lung cancer is four times higher than someone pre-pandemic.
But wait! It gets worse! If you get re-infected, your risk goes up some more. Compared to patients with one COVID-19 infection, patients reinfected patients had an additional higher risk:
| Disease | Increased Risk |
| Asthma | 3.00x |
| COPD | 3.07x |
| Any interstitial lung disease | 3.61x |
| Lung cancer | 3.20x |
This paper from China (2024-02-01) found that healthcare workers who had mild COVID-19 infections had worse cognitive function than healthcare workers with no COVID-19 infections. The COVID-19 group scored slightly worse on measures of attention, and quite a bit worse on measures of executive function. Functional MRI (fMRI) measurements found that the COVID group had diminished activity in two parts of the brain (left superior and left middle frontal gyri).
This paper using data from South Korea (2024-03-05) found that people who had COVID-19 were 25% more likely to be diagnosed with an autoimmune inflammatory rheumatic disease in the next year than healthy controls; they were 30% more likely to be diagnosed than people who had been infected with influenza. (Say it again for the people in the back: COVID-19 IS NOT THE FLU!)
The paper also found that the risk of an autoimmune disease diagnosis dropped to normal after one year, and that vaccines helped reduce the risk (although they didn’t say by how much).
Vaccines
This Correspondence from USA (2024-03-04) found that boosting with one of the XBB.1.5 vaccines (Pfizer and Moderna) had a vaccine effectiveness of 31% against hospitalization/ED compared to people who did not get a booster. Against death, XBB.1.5 vaccination was 42% effective compared to those who did not get a booster.
This case study from Germany (2024-03-04) describes a man who got 217 vaccine doses of eight different types.
For most of the doses, other people paid him to take their shots for them, but there were four which he got after he was busted. (Three of four were strain-specific boosters which he would just be normally eligible for, and the fourth was GSK/Sanofi, and I don’t have an explanation for that one.) The ones he took during the fraud period were mostly COVID Class-based mRNAs, but he also got one J&J and five AZ.
This puts my mind at ease that my seven doses of six types is not going to screw me up. 🙂
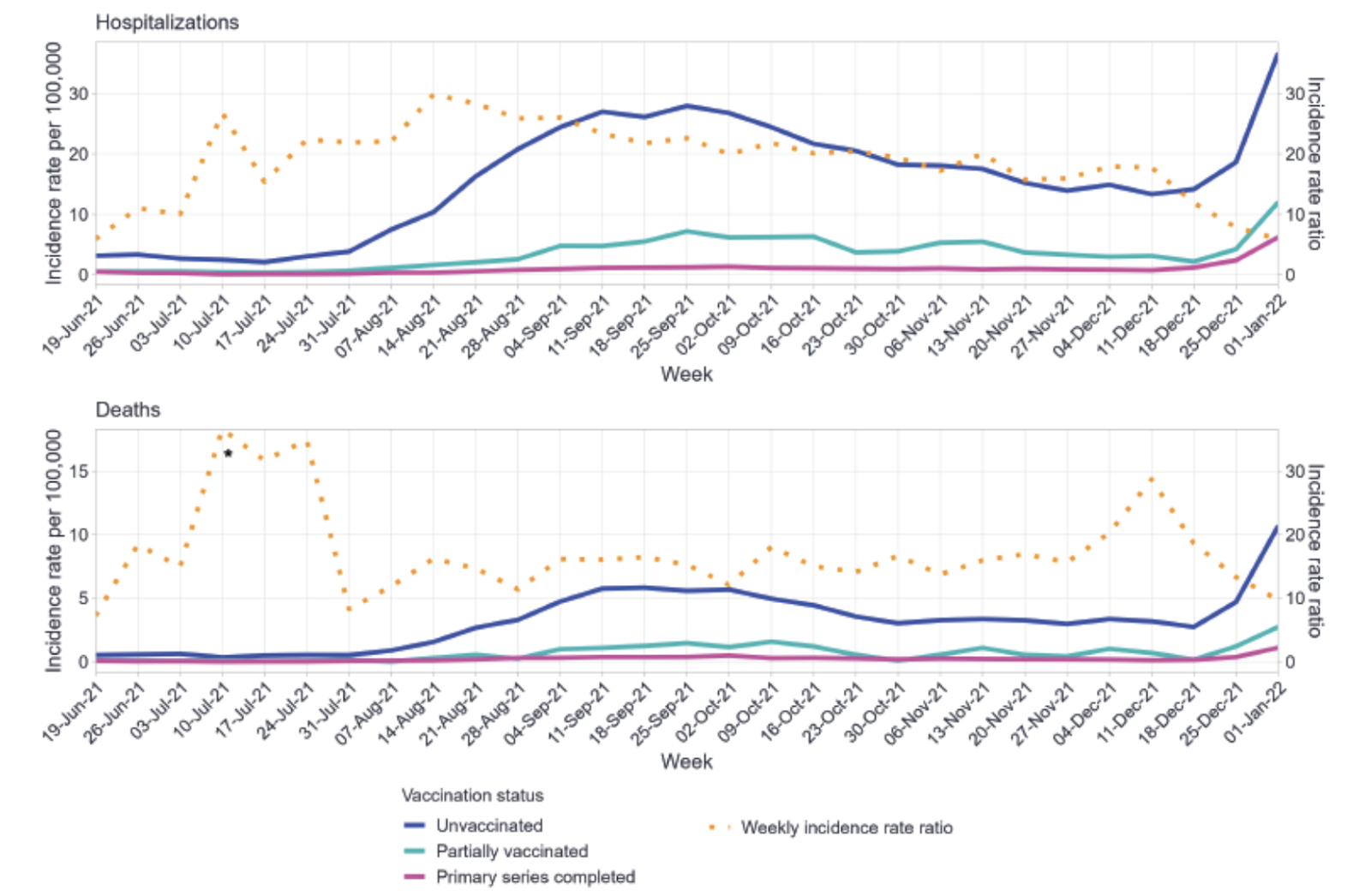
This report from PHAC (2024-03-04) found (no surprise!) that vaccinated people get sick and/or die much less than unvaccinated people.
During Delta, unvaccinated people were 6.8x as likely to get infected, 11.4x as likely to be hospitalized, and 17.5x as likely to die. During Omicron, unvaccinated people were 0.9x as likely to get sick, 7.1x as likely to to get hospitalized, and 11.3x as likely to die.
This article from USA (2024-03-04) reports that the US CDC director said that they expect next fall’s COVID-19 vax to be based on a different strain (presumably whatever is circulating this summer). I mention it because Canada usually says, “Oh, I’ll just have what the US is having.”
Treatments
This paper from USA (2024-04-04) found that nirmatrelvir (the important ingredient in Paxlovid) was 39% effective against severe outcomes, while molnupiravir was 50% effective against severe outcomes (compared to standard care for both). Against death, nirmatrelvir was 88% effective and molnupiravir was 87% effective.