
Because the rest of the world has decided that COVID doesn’t exist any more, I am dropping down to one post per week.
I am going to stop posting articles which are repetitive, especially ones of the form
- “Oh look! {Vaccines, boosters, treatments} still work against {Omicron, older variants}”;
- “Oh look! Vaccines wane in effectiveness!”;
- “Oh look! Myocarditis from vaccines really is almost always no big deal!”;
- “Oh look! Four doses are better than three!”. (For elderly and clinically extremely vulnerable who got their third shot more than six months ago, I think the data is unequivocal: do it NOW. For younger people who got their shot within six months, I personally think it would be better to wait, on the grounds that a booster seems to last about six months, so have your clock start later.)
- “BA.2 has roughly the same as immune-evasiveness as BA.1”.;
Testing
Awesome!! This article says that the US FDA approved what is basically a breathalyzer for COVID-19. It apparently did really really well in trials; here’s hoping that Canada approves it soon. It would be awesome for e.g. hospitals. (It would be nice if you could also put it in bars and restaurants, but apparently it has to be operated by a trained health care professional.)
Pathology
This paper found that COVID-19 RNA was found in people’s poo for a surprisingly long time. The percentage of people who had fecal RNA was:
- 49.2% in the first week;
- 12.7% after four months;
- 3.8% at seven months.
Not only that, but having COVID-19 in your poo correlated with unpleasant gastrointestinal symptoms.
This highly technical paper (i.e. “Ducky did not understand it completely”) seems to say that SARS-CoV-2 damages cells just by entering the cells. Complications ensue.
This article says that people with Down Syndrome are ten times more likely to die from COVID-19, and it might be in their genes. People with Down Syndrome have an extra copy of chromosome 21 (or a part of it), and there are some genes on chromosome 21 which relate to inflammation and TMPRSS2 (which turns on an enzyme which helps SARS-CoV-2 enter cells).
Huh. This article (from 2020) says that 11.7% of people who were hospitalized for influenza had acute cardiovascular events. Maybe it’s not the COVID-19, it’s the hospitalization? Or just viruses in general?
Transmission
I have been seeing chatter on Twitter about UV-C as a way to kill viruses in the air. (Here’s an article which talks about a nice experiment in 1956 which simultaneously proved that tuberculosis was airborne and that UV-C could kill it.) UV-C is nasty; I’ve seen some people saying that you put it far enough away from humans (but still in the airstream) that it doesn’t bother the humans; this article from June 2020 says that far-UVC light (207–222 nm) doesn’t bother humans but does bother COVID-19. Stay tuned on this.
This study asserts that “children were an important source of spread” in households, but their study actually said that adults were more dangerous. They found that adults were 2.2x as likely to spread to other household members as kids, and kids were 1.2x as likely to spread it to other kids than to adults.
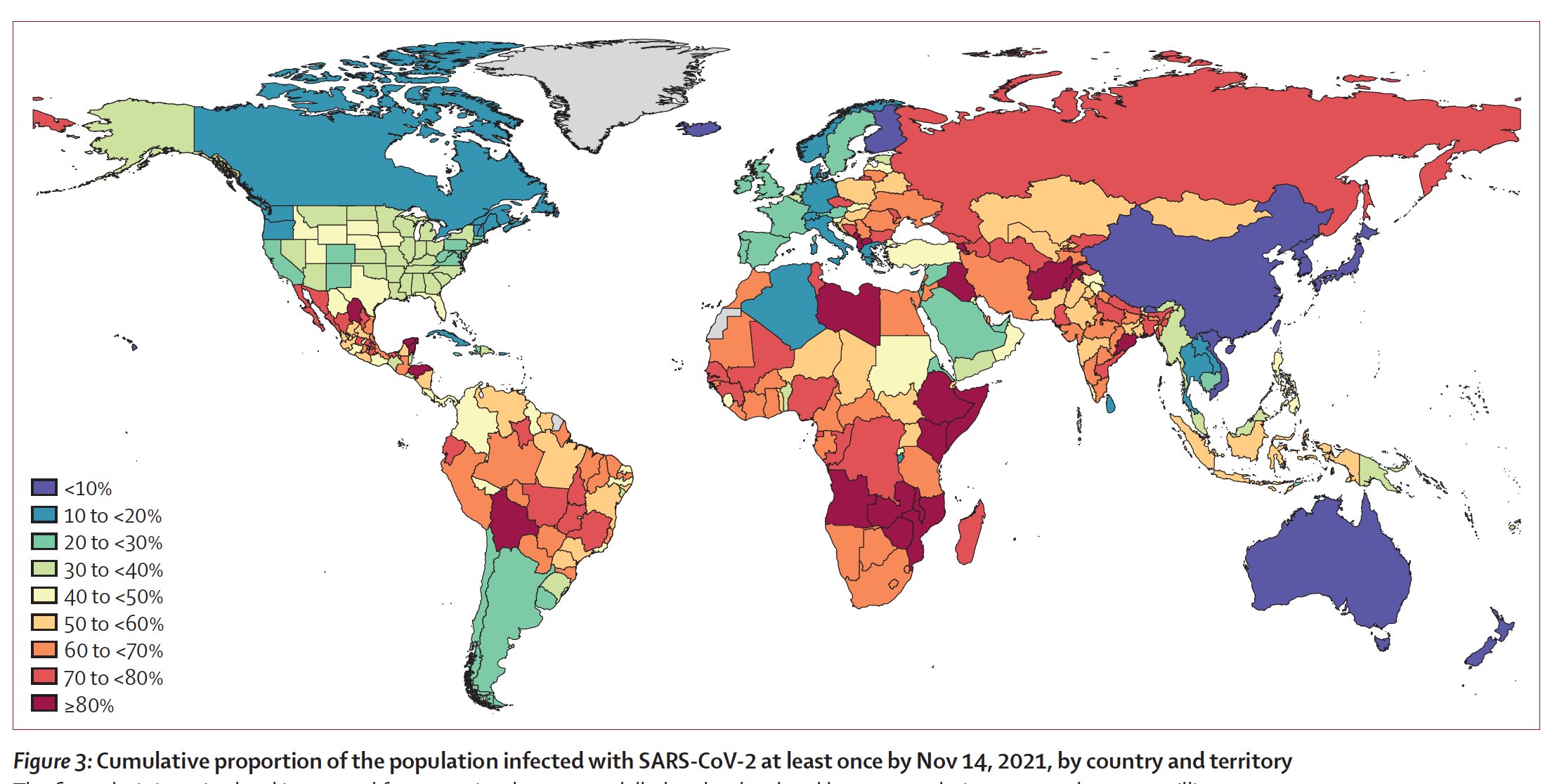
This paper estimates that 43.9% of the world’s population had COVID-19 at least once by November 2021 — which was before Omicron.
Treatments
This article says that the Government of Canada approved Evusheld today. Evusheld is a monoclonal antibody that works sort of like a vaccine: one shot and you’ve got antibodies for six months. It is particularly useful/important for immunocompromised people. (Some immunocompromised people can mount some defence after enough shots, but there are some who make pretty much zero antibodies.)
This article says that a new COVID-19 treatment, sabizabulin (a breast cancer drug in Phase 2 trials), reduced deaths of people who were already in the hospital with severe COVID-19 by 55%. (They stopped the trial early because the results were so good!)
This drug is important because the other treatments generally need to be given very soon after the patient is infected — once they get very sick, it’s too late. And, the people who don’t really believe in COVID-19 are the most likely to not get vaccinated, to get sick, to not get tested, and so not know they are sick until it’s too late for Paxlovid or Molnupovir.
In this small study, 13% of BA.1 patients who were treated with Sotrovimab developed mutations which reduced its effectiveness.
Vaccines
The Government of Canada has 18M doses of vax on its shelves, but it’s starting to expire. 1.5M has already expired, and most of the rest will expire in the next four months. (Even the 3.1M doses of Novavax which we just got is going to expire in August.) This doesn’t even count the 10-12M that the provinces are sitting on.
Canada also has only donated 15M of the 38M that it promised it would deliver, although that is not entirely Canada’s fault. COVAX has moved from getting vaxes “pushed” at it to “pulling” vax when it wants vax, and the distribution channels aren’t distributing the doses as fast as one might like.
This recent preprint, this paper from September 2021, and this paper from August 2021 all made frankenvaccines ahem mosaic vaccines with proteins from a bunch of different coronaviruses, then tested them in animals (mice and/or monkeys). They found that mosaic vaccines did better across a wide range of infectious coronaviruses than SARS-CoV-2-only-targeted vaccines.
This review article found that the rate of myocarditis was broadly similar between COVID-19 and non-COVID-19 vaccines overall. They found that the risk was a bit higher in mRNAs than non-mRNA COVID-19 vaccines, and the risk was WAY higher for smallpox vaccinations.
This paper found out several things about viral load and COVID-19:
- Vaccination reduced viral load in infected people;
- people infected with COVID Classic had lower viral load than people infected with Delta;
- people with Omicron breakthrough cases had about as much viral load as unvaccinated people if they only had two shots, but those with a booster had much lower viral load;
- viral load was lower in people who had Omicron than those who had Delta.
This paper says that there is no evidence yet that T cells get “stuck in a rut” from repeated infections or vaccinations; they still maintain a good diversity.
This paper — if I understood it properly — has found a good correlate of protection for vaccines. In other words, they ought to be able to test vaccines in about two weeks with a small number of people, instead of it taking months with huge numbers of people. If it is what I think, it’s great news!
This article says that the UK has approved Valneva — an inactivated whole-virus vaccine — for emergency use. I suspect that approval will be very slow in Canada; it was approved based on antibody levels in test tubes, not on how many people died relative to controls. I just wanted to get it on your radar.
This article says that CoVac-1 — a peptide vaccine specifically designed to stimulate T-cells in people whose B cells have been depleted e.g. from chemotherapy — generated COVID-19 T-cell responses in 93% of patients with B-cell deficiencies. This is cool.
Variants
Oh great. 🙁 This paper says that VOCs are able to infect a wider range of non-humans than COVID Classic.
This report from the US says that they found ten people in four states who caught COVID-19 again after a previous infection less than 90 days before. (These reinfections were between October 2021–January 2022, so in the Delta to Omicron BA.1 timeframe.) One person had two shots but not three; the other nine were not “up to date” with their shots. My takeaway: get vaxxed! Get boosted!
Recommended Reading
This article talks about naming. Why doesn’t BA.2 have its own name?
This article talks about how the USA fumbled booster communication, but it’s relevant to Canada because so much messaging filtered north.