
This article reports that BC’s Ministry of Health will switch to monthly COVID reports after the May 2 update. I will obviously cut back on BC posts in the summer; I haven’t decided how much I will cut back on the General posts.
H5N1
H5N1 is starting to hit the news, and I will post interesting/important news about bird/cow flu as it comes up. Yes, this blog is titled “COVID-19 in BC”, but it’s my blog and I make the rules. (Maybe I’ll change the name of the blog/URL, but probably not any time soon.)
For what it’s worth, I think that H5N1 is not really a bigger active threat right now than it was one to four years ago. It seems unlikely to me that bird/cow flu in pasteurized milk is a big threat; I think the risk from bird feces is currently/still much higher than from cow milk. H5N1 does have the potential to be really really bad, but me, I’m still drinking milk — and avoiding bird shit.
Long COVID
There have been a lot of studies which I have seen that have found SARS-CoV-2 in patients who have recovered from the acute phase of COVID-19.
Recently, this paper from China (2024-04-22) found SARS-CoV-2 in liver, kidney, stomach, intestine, brain, blood vessel, lung, breast, skin, and thyroid samples. They found persistent virus in 30% of samples 1 month after acute COVID-19 onset, 27% after 2 months, and 11% after 4 months. They also found a ~5x higher rate of Long COVID in patients who tested positive for persistent virus than in those who did not have persistent virus.
Note that there are lots of diseases which maintain reservoirs of disease long after the initial infection. Genital herpes, chickenpox / shingles, Epstein-Barr virus, HIV, cytomegalovirus, and many others can persist for years — so this is not unprecedented.
This paper from Hong Kong (2024-04-23) found that they were able to predict Long COVID symptoms pretty accurately from the composition of long haulers’ gut bacteria.
This paper from USA (2024-04-23) found that people who had had COVID-19 infections had the same average score on a standardized taste test as COVID-free people a year after their infection. However, their average smell score after a year was slightly but significantly lower than controls. 30.3% of the COVID-infected cohort had at least some smell dysfunction at one year, compared to 21.0% of controls (a +64% increase).
(I want to know why 21% of controls have smell dysfunction!)
This paper from UK (2024-04-17) found that men with Type 2 Diabetes (T2D) had a 17% higher risk of Long COVID than controls, while women with T2D had a 13% lower risk of Long COVID than controls.
Interestingly, the prevalence of Long COVID in men and women with T2D wasn’t much different. This is different from most studies I have seen, which find more women than men. Maybe women go get treatment (and diagnoses) while men just “tough it out”?
COVID-Related Excess Death and Sickness
This paper from Canada (2024-04-20) found that people with existing neurological issues were at a higher risk of death if they had a positive COVID-19 PCR test early in the pandemic:
| Pre-existing condition | Increase in Risk of Death w/COVID |
| parkinsonism | 1.65x |
| dementia | 1.30x |
| seizures | 1.91x |
| encephalopathy | 1.82x |
| stroke | 1.75x |
| any issue | 2.32x |
In addition, they saw an increased rate of new neurological diagnoses among people who had tested positive for COVID-19 vs. those who had not:
| New condition | Increased Risk of Diagnosis w/COVID |
| encephalopathy | 2.0x |
| dementia | 1.36x |
| seizure | 1.77x |
| brain fog | 1.96x |
| inflammatory myopathy | 2.57x |
| coma | 1.87x |
This paper from USA (2009-10-01) found that people who were born in 1919 — those most likely to have been exposed prenatally to the Spanish Flu — were 25% more likely to have a heart attack after age 60 than people who were not born in 1919. They also had lower levels of educational achievement and were shorter. The effects were stronger for men than for women.
This study from Sweden (2019-08-19) also found increased mortality in the 1919 birth cohort. Additionally, they found that men in the 1919 cohort had higher rates of cancer and heart disease.
(Yes, this is flu and not COVID-19, but it gives an existence proof that serious diseases can serious long-term effects — like COVID-19.)
Transmission
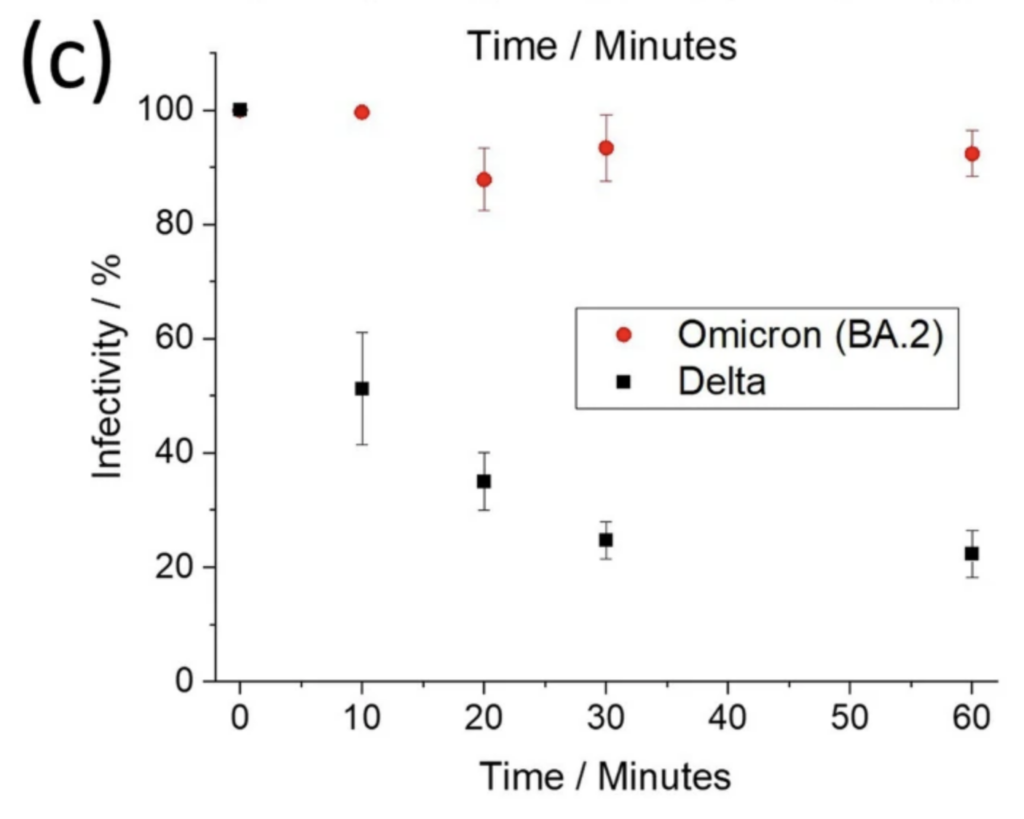
This paper from UK (2024-04-26) found that the stability of SARS-CoV-2 in aerosols went up as the CO2 level went up! They say that the effect of CO2 on infectiousness of SARS-CoV-2 is higher than the effect of humidity!
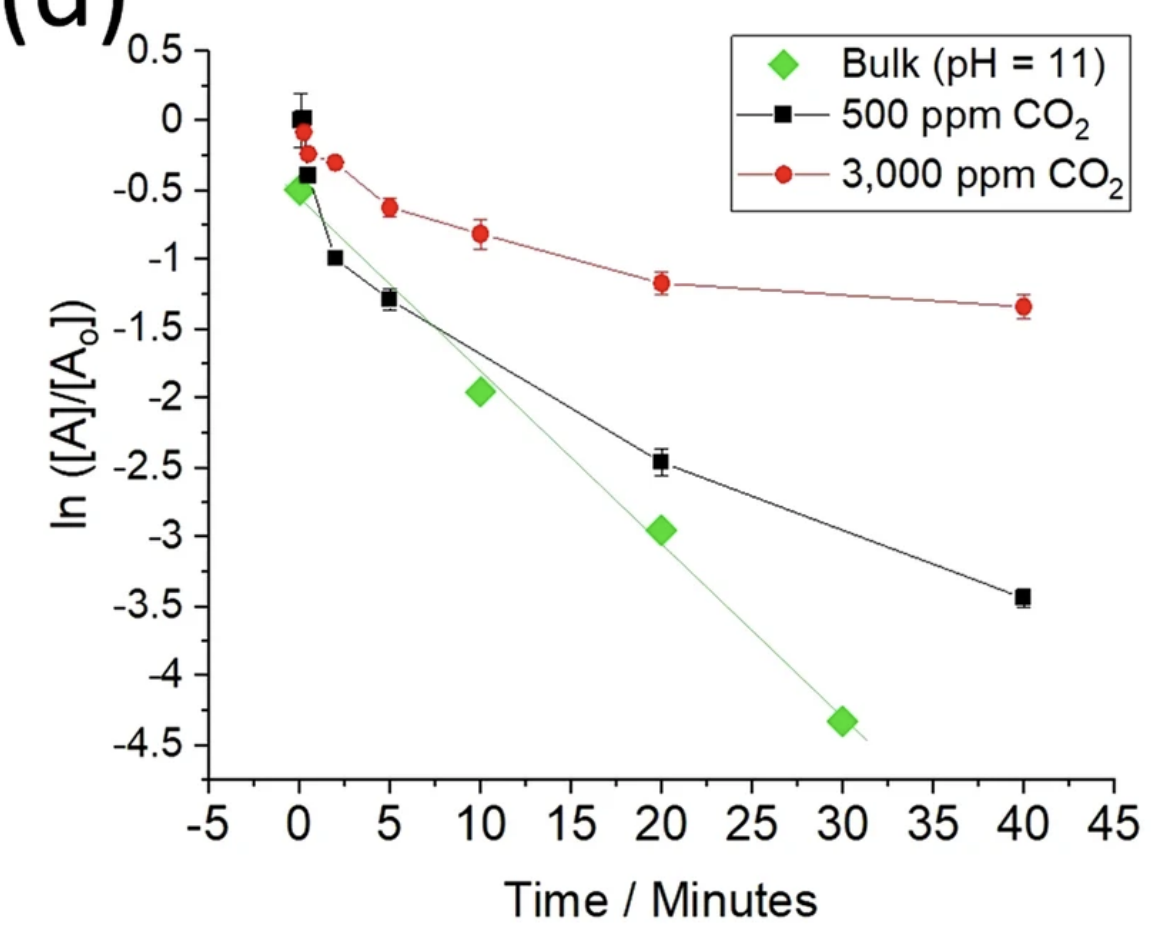
They also looked at the stability of different strains in the air. BA.2 was more a lot more stable in the air than Delta:

This paper from Denmark (2024-04-17) matched credit card transaction records with COVID testing records and compared people who made a purchase within five minutes of an infected person to people who made a purchase 16 to 30 minutes before the infected person. Based on the data they collected, they estimate that retail transmissions alone added for 0.04 to the R-value, and more during Omicron.
Treatments
This paper using Hong Kong data (2024-04-16) found that starting Paxlovid earlier than three days after symptoms start, gives a higher chance of rebound without reducing infectiousness; starting later than five days post-symptoms reduces its effectiveness. So start your Paxlovid between 3 and 5 days after you start seeing symptoms!
This paper from USA (2024-04-22) found that nasal treatment with the antibiotic neomycin strongly protected mice against COVID-19. Neomycin-containing Neosporin(TM) ointment in the nose was well-tolerated and effective at boosting the innate immune system in both mice and humans. Neomycin boosted the innate immune system after a day and for five days.
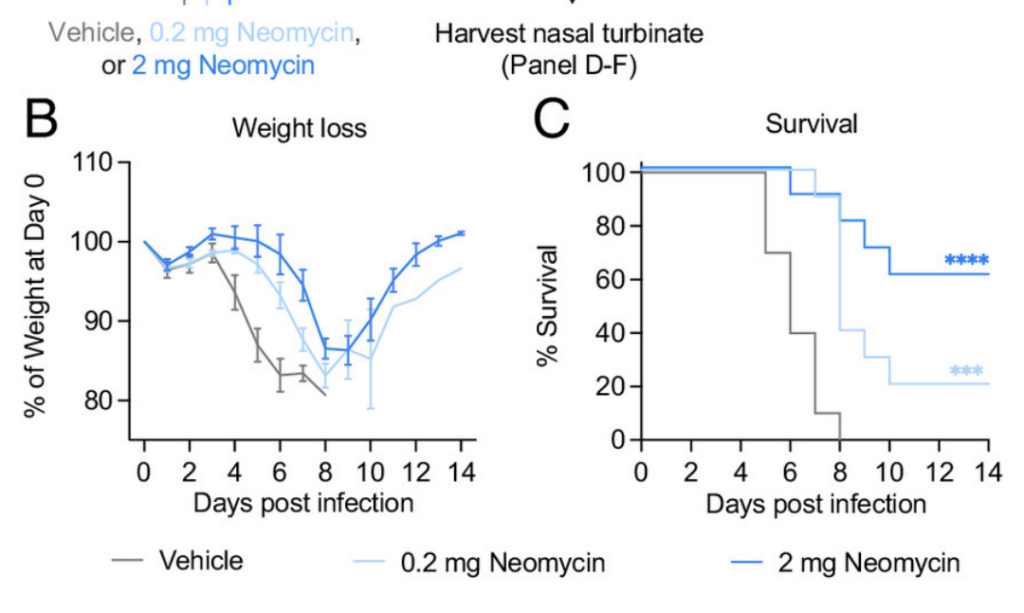
Now, I would not recommend immediately starting to put neosporin in your nose. It is an antibiotic, and as such kills bacteria — and we don’t yet know a lot about what bacteria are beneficial for the nose. This article reports that there might be bacteria that are beneficial for the nose.
Vaccines
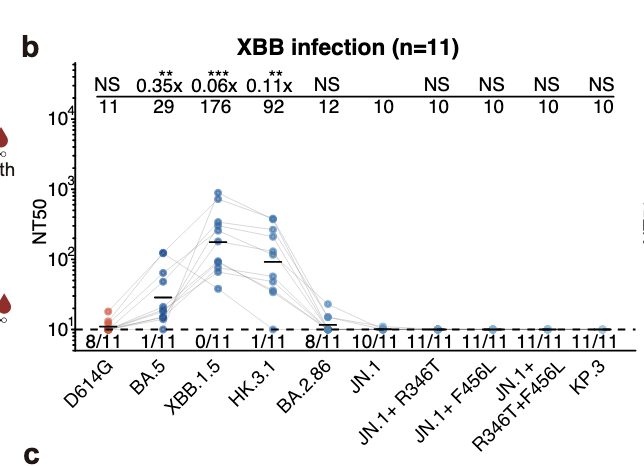
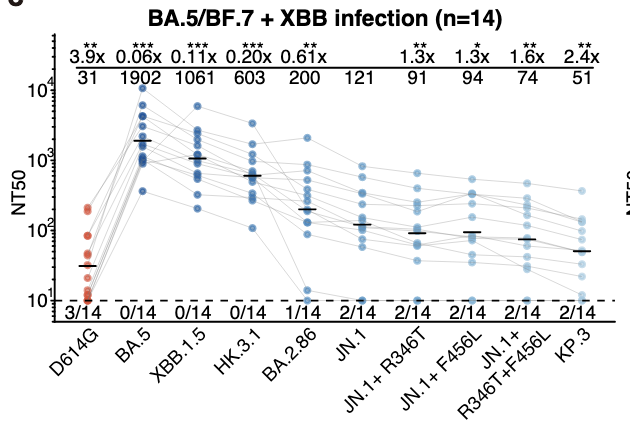
This paper from China (2024-04-22) was a bit confusing. It looked at infection with various combinations of infections and vaccinations. What they picked didn’t make much sense to me until I realized that China’s experience was very different from ours: they had relatively low rates of vaccination with COVID Classic-based vax, and then kind of “everybody” got BA.5 when China opened suddenly. So in this study, they made five cohorts with BA.5 infections plus all four combinations of with/without Classic vax, and with XBB 1.5/JN.1. They also had two cohorts of completely COVID-naive people (i.e. no vax, no infection) who then got an infection with either XBB 1.5 or JN.1. The authors then looked at how good the cohort’s antibodies were against currently circulating virus (including the strains with the FLiRT mutations, which many people are saying is going to be the next big thing (like this blog post).
The big takeaway is that if you only had an XBB 1.5 or JN.1 infection, than your protection against the other (JN.1 or XBB 1.5) was pretty crappy. If you had a BA.5 infection, then that helped a lot at boosting your protection against the FLiRTs (mutations R346T and L456L).
If you had a {COVID Classic shot + BA.5 infection + XBB infection}, then your protection is slightly worse than {BA.5 infection + XBB infection} against everything but COVID Classic, which probably is from “imprinting” on COVID classic.
Here are the graphs of how good the antibodies generated from each of those three cases are against various different strains (read my captions below the images, I think they are clearer)

The takeaway for me is that you want to get vax against all the different strains that you can in order to give you better protection against future variants. (I am assuming that vaccination against a strain is similar to an infection with a strain, which I’m pretty sure tracks with the research. I believe that vaccination against strain X gives better protection against strain X than infection with strain X, but that infection gives slightly better protection against future strains than an X-strain vaccination (but is much more dangerous).)
This article (2024-04-24) reports that the Government of Canada has added $36M to the vaccine injury fund. I’m all in favour of vaccine injury funds, but why are they topping up the original $75M when they have only paid out $11M? And why has the government paid an outside company $56M to disburse $11M? (The $11M maybe came from the $56M, but still…)
Testing
This paper from Kuwait (2024-03-25) found that the diversity of bacteria in saliva was predictive of the severity of COVID-19 cases.
Recommended Reading
H5N1: This article from USA talks about what it would take to make enough H5N1 flu vax for everyone. It’s tailored for a US audience, but realistically, that’s where we in Canada will get our vax from.
Me, I think it might make more sense to vaccinate all 90M cows in the US instead of waiting until it jumps to humans and then vaccinating 8B people in the world. :-/