
Public Service Announcement: Get your flu shot! This pre-pandemic paper from Canada (2018-01-18) reports that the risk of heart attack goes up by about TEN TIMES in the week after an influenza B infection compared to the year before and year after. (Influenza B is much less common than influenza A, fortunately.) Other respiratory diseases also up your risk significantly in the week after infection:
- Influenza B: 10.11x
- Influenza A: 5.17x
- RSV: 3.51x
- Other respiratory viruses: 2.77
This recent large study from Netherlands (2024-06-25) agrees that flu is bad for your heart: they found that risk of heart attack in the week after a flu infection was about six times greater than the year before or 51 weeks after. (NB: They didn’t break influenza A and B out separately.)
Long COVID
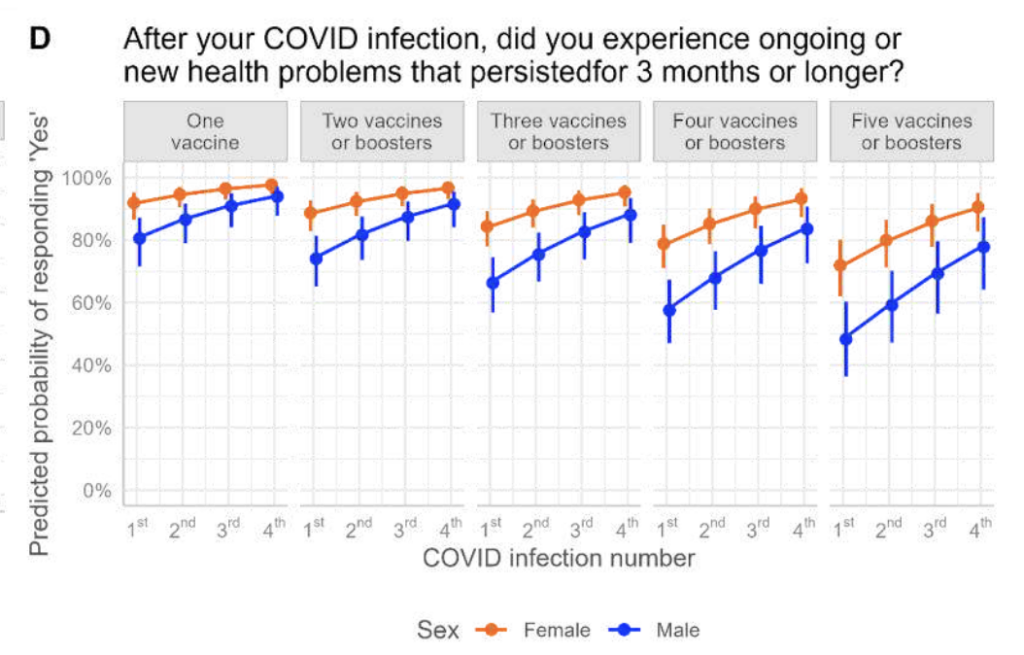
This preprint (2024-09-24) reports that repeated COVID-19 infections increase the risk of Long COVID. A second COVID-19 infection increased the risk of Long COVID by 2.14 times; a third COVID-19 infection increased the risk by another 1.75 times.
The risk of Long COVID went down the more vaccines people got — especially for men — but the protection diminished the more infections people had.
This article (2024-09-24) discusses a paywalled paper from UK (2024-09-23) which reports that hospitalization for COVID-19 causes cognitive issues that “look similar to 20 years of normal aging”. It was worse for people who had worse acute COVID, those who had post-acute psychiatric symptoms, and who had had a history of encephalopathy (various diseases of the central nervous system). There was one piece of good news: long-term followup “pointed to a trend toward recovery”.
This paper from USA (2024-09-25) reports that vaccines help reduce Long COVID in health care workers, at least at the six-week mark. Health care workers who had two shots plus a booster booster before they got a COVID-19 were 45% less likely to have symptoms at six weeks than people who just got two shots. If the booster was less than 16 weeks before the infection, the people were about 31% less likely to get any symptoms than if the booster was more than 16 weeks prior to the infection.
This study also looked at prevalence, with a control group. They found that 26% of the people had symptoms at six weeks, but 18% of the people who did not get COVID-19 also had symptoms, which I take to mean that about 13% of people’s symptoms came from COVID-19.
Fatigue and difficulty sleeping were the symptoms most closely correlated with COVID-19.
This article from Japan (2024-09-23) reports that 15.0% of people who had a COVID-19 infection got Long COVID symptoms, while only 4.4% of people who did not get a COVID-19 infection got Long COVID symptoms. They also found that the risk of Long COVID dropped over time: 27.0% of COVID-infected people got Long COVID during the Alpha and Delta waves, while only 12.8% got Long COVID during the Omicron wave.
Vaccines dropped the risk of Long COVID by 71% in the Alpha and Delta waves, but only by 21% in the Omicron wave.
Vaccines
Pregnant people, get a COVID vaccination! This report from US CDC (2024-09-26) found that infants were as likely to get hospitalized for COVID-19 as people aged 65-74 years old. Only the over-75 crowd was at greater risk.
This paper from China (2024-09-24) reports that an intranasal vaccine — a replication-incompetent adenovirus carrying Omicron BA.1 spike — worked really well in a Phase 2 trial in humans. (Phase 2 trials are smallish, and designed to study safety, not effectiveness, but of course they look anyway.) The vaccine caused really high nasal IgA levels, and didn’t wane too badly.
The trial started right before China gave up on it’s Zero COVID strategy, and unfortunately more than half of the participants caught COVID-19 after the first dose but before the second dose. However, nobody — zero people! — got sick after the second dose for the length of the study (which ended 90 days after the second dose).
This paper from USA (2024-09-24) reports that COVID-19 vaccination (with mRNA vax) does not produce long-lived plasma cells (LLPC) in the bone marrow. They studied the blood of volunteers 2.5 months to 33 months after a COVID-19 mRNA vax, and found that the blood had plenty of LLPCs for tetanus and influenza (presumably from previous vaccination or infection), but almost no COVID-19 LLPCs. People who had had COVID-19 infections also didn’t make LLPCs for COVID-19. I presume this is part of why COVID-19 vaccines don’t prevent symptomatic or asymptomatic infection very well. (Here’s a thread explaining the paper.)
Addendum 2024-10-10: This blog post gives a very detailed takedown of the paper. In particular, the blog author takes issue with the way the paper authors excluded certain cells from the counts of possible COVID-19 LLPCs. The blog post also points out that maybe it doesn’t matter: the paper found LLPCs for influenza, yet people get influenza over and over.
Treatments
Wow! This paper (2024-09-24) reports that a nasal spray called Pathogen Capture and Neutralizing Spray (PCANS) is remarkably effective at protecting mice from viral pathogens. They dosed up some mice with 25 times the lethal dose of influenza, and 0% of those mice died, compared to 100% of undosed controls. Furthermore, it uses no drugs — only stuff that is on the US FDA’s Inactive Ingredient Database and Generally Recognized as Safe list — making a gel that coats the nose! That means that it could get approval really fast (if it even needs approval, I’m not sure). The mice presumably did not give feedback on how comfortable it is to have a gel inside your nose.
While the mice mortality testing used influenza, the authors also did test-tube studies that say it also works with SARS-CoV-2, RSV, adenovirus, and K Pneumonia.
The paper is paywalled except for an abstract; here’s a thread reader synopsis.
Recommended Reading
What repeat COVID infections do to your body. (Hint: COVID-19 is not the flu.)
This article from US (2024-09-25) looks at Paxlovid vs. metformin, especially in protecting against Long COVID. Tl;dr: metformin wins, especially among young (i.e. not elderly) people.
H5N1
Transmission
This press release (2024-09-27) reports that four more healthcare workers who were in contact with the index human H5N1 case have had mild respiratory illnesses (and recovered). Testing has not yet been completed on six of the seven contacts with illness. (One was confirmed negative for bird flu.)
You would think that they’d have the testing done by now, but this article (2024-09-30) says that getting the samples to CDC Atlanta was delayed by hurricane Helene.
This US CDC press release (2024-09-27) reports that 238 dairy herds in 14 U.S. states have confirmed cases of avian influenza A(H5N1) virus infections in dairy cows.
Mpox
Transmission
You might recall that there was an mpox outbreak of clade 2b (the less fatal one) a year ago, which mostly died down. This paper (2024-09-18) found that it died down more due to high-risk groups (mostly men who have sex with men) cut down on risky behaviour than due to vaccination.
Unfortunately, that’s probably not going to help up with the current clade 1 outbreak. This commentary (2024-09-18) points out that children account for 66% of cases and 82% of the current mpox outbreak’s deaths in DR Congo. We probably are not going to be able to greatly reduce the amount of sex that children have.
Meanwhile, 29% of cases in DR Congo are from sex workers, and it’s hard to avoid sex when it’s your livelihood. 🙁