
COVID-19
I’m going to put stars ⭐ next to papers that I think are particularly exciting.
My Bad!
I have, in the past, referred to the nucleocapsid as the “ball” part of the spiky ball that is a SARS-CoV-2 virion. I was wrong: the “ball” part is called the “envelope”. Inside the envelope is the nucleocapsid, and inside the nucleocapsid is the virus’ genetic code. (No, I still don’t fully understand what purpose the nucleocapsid has that the envelope doesn’t provide.)
Long COVID
This paper from UK (2024-08-28) reports on a large Long COVID survey of health care workers four months after they got COVID-19 infections.
- 32.7% had persistent symptoms after their first infection;
- 21.6% had persistent symptoms after their second infection;
- 21.6% had persistent symptoms after their third infection.
They also saw a difference between strains: 52.9% had persistent symptoms after COVID Classic, while only 20.7% had persistent symptoms after Omicron.
There was also a difference due to vaccination: 38.1% of the unvaccinated people had persistent symptoms, compared to only 22.0% of the vaccinated people. (NB: Vaccination cutting your risk in approximately half is consistent with other studies I’ve seen.)
24.0% of the people with persistent symptoms reported that the symptoms impacted their day-to-day live “a lot” and 14.4% reported that it impacted their work “a lot”. 8.9% said they had reduced their work hours and 13.9% said they had changed their work patterns.
One thing to note is that variant, vaccination, and infection number are not independent variables. A lot more people caught Omicron in 2022 than caught COVID Classic in 2022; a lot more people were vaccinated in 2022 than in 2020; and a lot more people got their first infection in 2020 than got their third infection in 2020. This means it is a little hard to tell why, for example, fewer people had persistent symptoms after Omicron than after COVID Classic: was it variant, vaccination, or number of infections?
This paper from UK (2024-08-28) is one of the only ones that I have seen that looked at the intensity of Long COVID symptoms in addition to the type of symptoms. They said that of the 109 symptom categories patients had, the top four were:
- pain – 26.5%;
- neuropsychological issues – 18.4%;
- fatigue – 14.3%;
- shortness of breath – 7.4%;
They found that the intensity of the symptoms got worse over time — 3.3% per month, and the intensity level varied by patient type:
- People 68 to 77 had 32.8% higher intensity symptoms than people 18 to 27;
- People 78 to 87 had 86% higher intensity symptoms than people 18 to 27 (OUCH!);
- Women had 9.2% more intense symptoms than men;
- Non-white people had 23.5% more intense symptoms than whites;
- People with higher education levels and wealthier people had less intense symptoms than lower-educated or poorer people.
COVID-Related Excess Sickness and Deaths
This paper from Switzerland (2023-06-13) reports that people who got COVID-19 infections early in the pandemic had worse ability to recognize emotions of people in pictures.
- People who had moderate respiratory symptoms were less able to recognize fear than people with mild respiratory symptoms;
- people who had severe respiratory symptoms were less able to recognize disgust and irritation;
- overall, poor performance correlated with decreased episodic memory and smell dysfunction.
Transmission
This preprint (2024-08-26) reports that the most COVID-cautious countries (Australia, China, Japan, New Zealand, South Korea) got more Olympic gold medals than would be expected, while the highly COVID-incautious countries (e.g. US, UK) got fewer than would be expected. This was not true for bronze or silver.
Pathology
⭐ This paper from USA (2024-08-30) reports that obese patients with pre-existing cardiovascular (CV) disease who took semaglutide (brand name Wegovy, a weight loss drug that does a lot of other things) were less likely to die over the course of ~3 years than obese CV patients were. Compared to obese CV patients who did not take semaglutide, ones who did were:
- 19% lower all-cause mortality risk;
- 15% less likely to die from CV disease;
- 23% less likely to die from a non-CV disease (mostly infectious diseases, which I suspect is mostly COVID-19).
Semaglutide didn’t change the risk of catching COVID-19, but it significantly reduced the risk of dying. Among patients who caught COVID-19, compared to ones who did not take semaglutide, the ones on semaglutide had:
- 26% lower risk of all-cause death;
- 17% lower risk of CV disease-caused death;
- 33% lower risk of dying from COVID-19.;
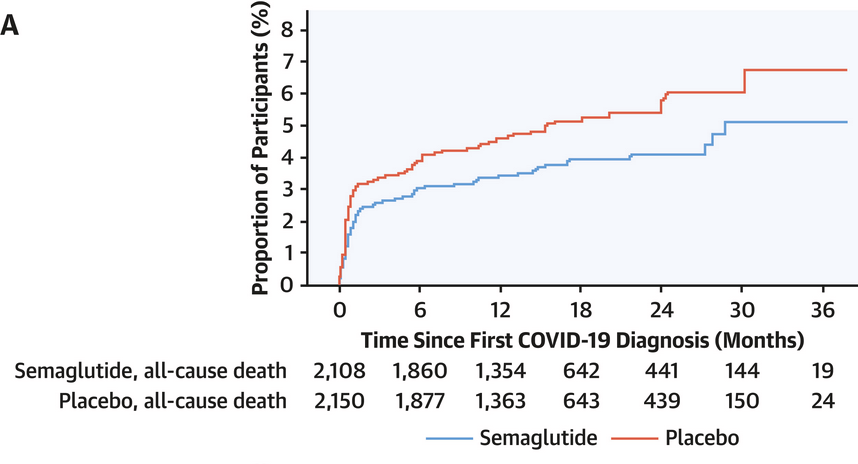
The reduced risk came immediately upon starting semaglutide, before any significant weight loss happened, so it’s not just “fat bad”. (It’s almost like obesity is a disease and not a moral failing, who knew?)
Metformin, another metabolic drug (an anti-diabetes drug), also significantly helps obese people against COVID-19 (see for example this paper that shows metformin drops the risk of death by 66%), so there is something important going on with metabolic processes and COVID-19.
This paper from USA (2024-07-23) found that SARS-CoV-2 caused human epithelium tissues grown in test tubes to lose the Cystic fibrosis transmembrane conductance regulator (CFTR). The drugs digoxin, digitoxin and ouabain prevented CFTR loss, so are very promising treatments for severe COVID-19.
Meanwhile, this paper from USA (2024-08-27) reports that obese people exposed to COVID-19 are 34% more likely to catch COVID-19 than non-obese people. They looked at people who got a COVID-19 PCR test before 2021 January 25 (before vaccinations were common) and who self-reported exposure to a person with COVID-19; the study found that obese patients were 34% more likely to test positive than non-obese patients.
It’s not clear to me if ⭐ this paper from USA (2024-08-28) should be under Pathology, or Long COVID, or Treatments.
¯\_ (ツ)_/¯
The paper reports that SARS-CoV-2 promotes blood clots, explains the mechanism, and gives a treatment. One of the hypotheses for Long COVID is that there are blood clots which interfere with oxygen transport, so this might be the mechanism!
From studies they did with mice, they found that spike protein binds to fibrinogen, a protein which is normally floating around in the blood, minding its own business. When there is an injury (in this case, COVID-19), thrombin shows up and converts the fibrinogen to fibrin, which makes blood clots. The spike protein also binds to fibrin, which makes the clots more durable, so they don’t break down as fast as they are supposed to.
In addition to making clots, fibrin also increases inflammatory processes and this study says that COVID-19 makes it increase even more.
The good news: when they gave the mice a known fibrin inhibitor, COVID-19 didn’t make them as sick! The fibrin inhibitor (called 5B8) prevented SARS-CoV-2 from binding with the fibrinogen or fibrin, so the clots behaved like they were supposed to. This prevented the extra inflammation from happening. 5B8 also reduced the amount of fibrin deposits / neural damage that they found in the brain.
They gave COVID-19 to some mutant mice which made fibrin but without the piece which increases inflammatory response, and those mice did not get as sick as the controls.
They also found that fibrin reduced the amount of Natural Killer (NK) cells that were produced. More NK cells means better, y’know, killing of viruses.
They also also found that fibrin reduced a lot of processes, including some related to mitochondria / energy metabolism. (Huh, I wonder if this is why you get tired when you are sick?) They didn’t say that the mice got tired, but mice are hard to interview about that.
You might ask why, if the spike protein binds with fibrinogen and causes a cascade of bad things to happen, why don’t the vaccines cause a similar bad cascade? I think the most important reason is that the vaccines don’t go into the blood. They go into the muscle, which drains into the lymph nodes, not the blood. That means that there is a lot less spike in the blood after vaccines than after infections.
Vaccines
This press release from USA (2024-08-30) says that the US FDA has approved the Novavax JN.1 booster. As I mentioned last week, Health Canada probably isn’t going to buy any Novavax, so you might need to go to the US if you want to get the JN.1 booster.
This paper (2024-08-26) is not of immediate applicability, but is interesting. It reports on a novel, nasally administered, live attenuated COVID-19 vaccine that they say works well across variants. The advantage of using a live virus is that the immune system gets to look at all parts of the virus, not just the spike. The disadvantage with live viruses is that the live virus can sometimes make people sick, which is why they attenuate them — to make them not dangerous. This paper uses a method that I had never heard of to attenuate the virus: codon deoptimization.
Codons are little three-genetic-letter sequences of DNA which instruct the cellular machinery what protein to make. However, there is not a one-to-one correspondence. There are 64 different codons, but those only make 22 proteins (plus one STOP codon and one START codon).
The cellular machinery needs pieces called Transfer RNA (tRNA). Each tRNA molecule has receptors for one codon on one side, and the corresponding amino acid on the other side. Those plonk down their codon side on a piece of messenger RNA, which puts the amino acid in the right place to join up with the previous amino acid:
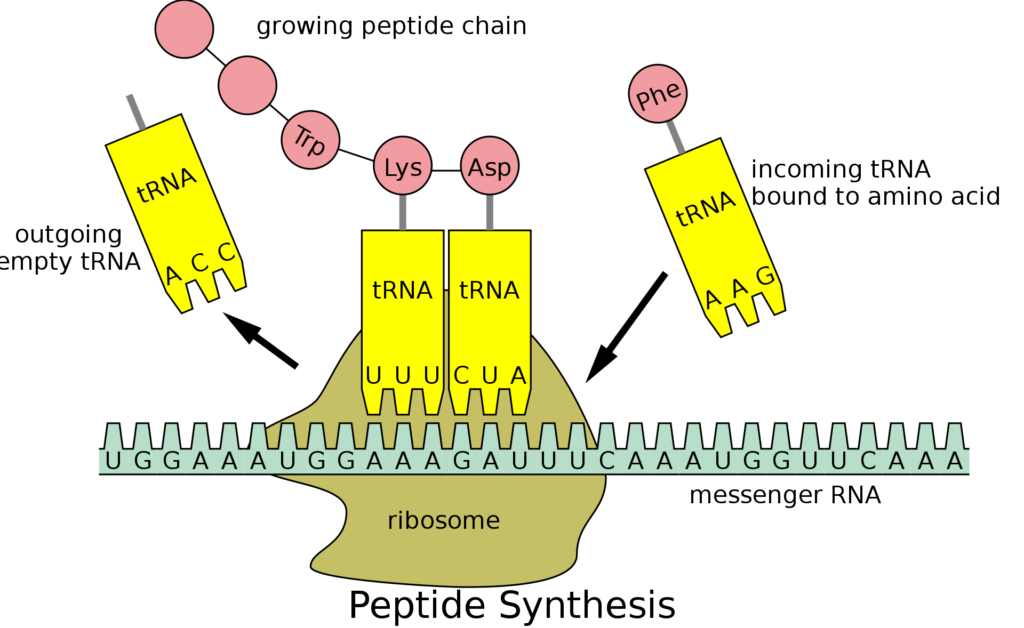
The key here is that any given animal’s cells have different amounts of the different tRNA molecules. Like there might be lots of molecules that have receptors for the ACC codon, but not many for the AGG codon. The proportion of tRNA types varies by species.
Back to the paper. To attenuate their version of SARS-CoV-2, they mucked with its RNA so that it had lots of codons that humans don’t have many tRNAs for. That means that their version of SARS-CoV-2 looks just like a regular SARS-CoV-2 virion, but it isn’t able to reproduce very fast, because the cellular machinery just can’t get the raw materials very fast.
This gives the immune system a chance to come up to speed on how to kill SARS-CoV-2 faster than SARS-CoV-2 can infect cells. Pretty slick.
When hamsters, mice which have human ACE2 receptors, and monkeys were immunized nasally with this codon deoptimized vaccine, they were very well protected, against multiple COVID-19 variants, with blood levels of good immune stuff that was quite stable for a long time. While there was waning over the course of a year, it was less than the standard mRNAs suffer from.
This paper with data from multiple European countries (2024-08-15) found that the XBB 1.5 vaccines had reasonable effectiveness in a period when XBB 1.5 lost dominance, but waned fast. The vax had an effectiveness of 69% for the first month but only 40% in the third month.
This paper from UK (2024-08-23) found that pregnant women during roughly the first year that COVID-19 vaccines had been approved were more likely to be admitted to hospital if they were unvaccinated. Hospitalized women were 78% more likely to be unvaccinated than vaccinated, despite 57% of the women being vaccinated.
Mental Health
This paper from Denmark (2024-08-23) reports that pandemic-related mental health issues changed over time in children between 8 and 16 years old between June 2020 and June 2021. Self-reported memories weakened over time in detail and emotional intensity. Emotional well-being decreased over time, with teenaged girls doing most poorly. Having memories which included more unpleasant and factual information about COVID-19 and lockdowns correlated with worse psychological well-being over time.
Treatments
This older paper (2024-01-25) reports that they have developed neutralizing nanoantibodies (antibodies that come from camelids which are about half the size of most mammal antibodies) which give 40-80% protection to mice modified to have human ACE2 receptors against COVID-19 when administered intranasally. These nanobodies also significantly reduced the viral load in the mice’s noses and brains.
Testing
This paper from Thailand (2024-08-30) reports on a very accurate COVID-19 test that uses collected sweat samples. They got >90% agreement with PCR tests by using a handheld photo ionization detector to measure underarm sweat samples. If the paper said how long each test took, I couldn’t find it, but the info page for the detector they used implied that a measurement took as little as 60 seconds!
Highly Pathogenic Avian Influenza
Transmission
This report from the US CDC (2024-08-29) describes culling operations at two Colorado poultry plants. 16.4% of the workers reported symptoms and agreed to be tested. Of those, 8.3% tested positive for H5Nx influenza (so probably bird flu) while 17.4% — more than twice as many! — tested positive for COVID-19!
This article (2024-08-30) reports that a herd in New Mexico was confirmed positive on 30 August — the state’s first since April. A herd in Michigan was confirmed positive on 26 August — the state’s first since July 26. The total number of ever-infected US herds is now 194 in 13 states.
Mpox
Vaccines
This paper from UK (2024-08-27) reports that the effectiveness of the Jynneos mpox vaccine (in England) against infection is 80% and against death is 100%.
Transmission
This press release from the World Health Organization (2024-08-26) announces details of their plan to stop mpox outbreaks. They think it will take USD$135M to implement the plan.