
This week’s postings will be short because I have Stuff To Do for the next few days.
COVID-19
Long COVID
This paper from USA (2026-01-27) reports that women who had both depressive and anxiety symptoms pre-pandemic and got a COVID-19 infection were 78% more likely to get Long COVID in 2020 and 2021 of the pandemic than women who got COVID-19 infections but did not have prior symptoms of depression and anxiety.
😛 This paper from Sweden (2026-01-29) reports that among a (small sample of) people with messed up taste a year after COVID-19, they didn’t have missing overall taste. Instead, about a third of them had dramatically reduced perception of one of more of the five tastes, usually losing sweet, umami, or bitter. (Sour and salty receptors usually still worked.) Sweet, umami, or bitter tastes are dependent on the enzyme PLCβ2 and protein Tas1R3.
My immediate thought was that these people could just eat some PLCβ2 and Tas1R3 with their meals, but looking more closely at the paper, I think that those proteins need to be inside the cells. The subjects’ taste buds usually looked fine, so maybe you could use mRNA injections to get instructions to make PLCβ2 and Tas1R3 into the cells. However, that seems like a lot of work and you probably would have to do it frequently. 🙁
COVID-Related Excess Death and Sickness
🤰 This paper from USA (2026-01-20) reports that babies who were exposed in the womb to COVID-19 had noticeable differences from babies who were not.
- Exposed babies had changes in brain volume in numerous areas of the brain: cortical gray matter, subcortical grey matter, cerebral white matter, and left hippocampus;
- exposed babies scored lower on tests of cognition and social emotional skills.
This is consistent with a bunch of other studies, and inconsistent with this paper from USA (2026-01-19) which I posted last week. That’s how science goes. ¯\_(ツ)_/¯
This paper from Singapore (2026-01-25) reports that early administration of monoclonal antibodies did not reduce Long COVID, but it did raise the risk of autoimmune diseases by 120%, especially lupus and rheumatoid arthritis.
Vaccines
💸 This article (2026-02-02) reports that Canada’s Vaccine Injury program has spent at least $34 million on administration and only $18 million, and that $18 million only went to 234 people. This is shocking and a disgrace. We need a good vaccine injury program! Vaccine injuries are very rare, but if people think they won’t be taken care of if they do get one of those rare injuries, they will be less likely to get a vaccine. (That will make them more likely to get an infection injury, especially since those are relatively common!)
😳💉 Last week, I said that Alberta, among other things, made people sign up for vaccines a year in advance. That was incorrect. My bad.
AGAIN This preprint from USA (2026-02-03) reports (yet again) that COVID-19 vaccination is a lot safer than COVID-19 infection. Men who had a COVID-19 infection had a 4.5x higher risk of death than controls; women who had a COVID-19 infection had a 4x higher risk of death than controls. Inflammatory cardiac complications happened four times as often after infection than after vaccination.
Vaccination, on the other hand, was protective. Getting a COVID-19 vaccination gave men a 76% lower risk of a later major adverse cardiovascular event (MACE) and women a 69% lower risk. Even getting a vaccination after a COVID-19 infection helped: post-infection vaccination reduced the risk by about 37%.
This paper from Thailand (2026-02-02) reports that women who had a COVID-19 infection had a 23% higher risk of irregular menstruation than those who did not have a COVID-19 infection.
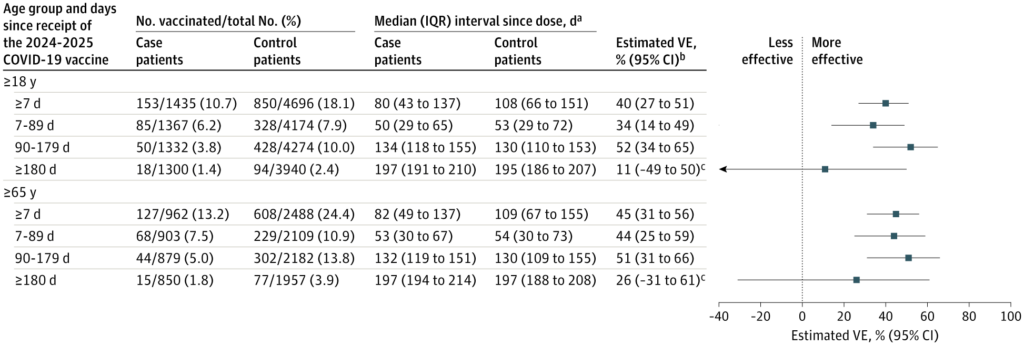
💉 This paper from USA (2026-02-03) reports on the effectiveness of the 2024-2025 COVID-19 vaccines (which were mostly probably Pfizer and Moderna):
- 40% against hospitalization;
- 79% against mechanical ventilation or death;
- 49%* against KP.3.1.1.;
- 34%* against XEC;
- 24%* against LP.8.1.
*Note that the time-since-vax increased as you went from KP.3.1.1 to XEC to LP.8.1 just because of what was circulating when. Thus it’s not clear how much the decline in effectiveness is from vaccine mismatch and how much is from the effectiveness waning over time.
They did also say that protection was good even up to 6 months, but it really fell off afterwards:
RSV
RSV-Related Excess Sickness and Death
This paper from USA (2026-02-03) reports that getting hospitalized with RSV significantly increases your risk of bad cardiovascular events. By a lot. (It’s almost like viruses are bad for you, who knew?)
| event | days 1-7 | days 8-14 | days 15-21 |
| myocardial infarction (heart attack) | 8.7x | 5.2x | 2.6x |
| stroke | 7.4x | 5.9x | 3.7x |
| congestive heart failure exacerbation | 12.5x | 4.1x | 2.4x |
| COPD exacerbation | 23.1x | 1.3x | |
| arrhythmia | 16.5x | 1.6x |
Measles
Transmission
According to the Government of Canada Measles and Rubella Monitoring Report (updated 2026-02-02), in the week ending 24 January 2025, the following jurisdictions had the following number of measles cases:
- Canada: 28;
- Manitoba: 20 (!);
- Alberta: 5;
- Nova Scotia: 1;
- Quebec: 1.
- BC: 1;